 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Nikola
Nikola Kayser
Kayser Fusion
FusionThinner Plantar Fascia Predicts Decreased Pain after Extracorporeal Shock Wave Therapy
- Type: Free
Thinner Plantar Fascia Predicts Decreased Pain after Extracorporeal Shock Wave Therapy
Huey-Wen Liang, MSc, MD*; Tyng-Guey Wang, MD*; Wen-Shiang Chen, MD, PhD*; and
Sheng-Mou Hou, MD†
Increased plantar fascia thickness is common with chronic plantar fasciitis, and reduction of the thickness after extra- corporeal shock wave therapy or steroid injection has been reported. We hypothesized a decrease of plantar fascia thick- ness was associated with pain reduction after extracorporeal shock wave therapy. Fifty-three eligible patients with 78 symptomatic feet were randomly treated with piezoelectric- type extracorporeal shock wave therapy of two intensity lev- els (0.12 and 0.56 mJ/mm2). Two thousand shock waves for three consecutive sessions were applied at weekly intervals. A visual analog scale for pain, the Foot Function Index, the Short Form-36 Health Survey, and ultrasonographic mea- surement of plantar fascia thickness were evaluated at base- line and 3 and 6 months after treatment. We analyzed the association between pain level and plantar fascia thickness with generalized estimating equation analysis and adjusted for demographic and treatment-related variables. Patients with thinner plantar fascia experienced less pain after treat- ment; high-intensity treatment and regular exercise were as- sociated with lower pain level. The overall success rates were 63% and 60% at the 3- and 6-month followups. High- and low-intensity treatments were associated with similar im- provements in pain and function. Receiving high-intensity treatment, although associated with less pain at followup, did not provide a higher success rate.
resonance imaging and echographic examination show thickening of the fascia in patients with plantar fasciitis. Extracorporeal shock wave therapy (ESWT) has been used to treat patients with chronic plantar fasciitis for the past 10 years. Its clinical effectiveness remains controversial despite the growing numbers of published studies that support its use. Furthermore, the optimal treat- ment regimen has not been well defined and the underly- ing mechanism of the treatment effect is unclear. Self- reported pain and function by questionnaire survey was the most frequently used outcome. One animal study suggests shock waves induce neovascularization,but its potential contributions to the direct reduction of pain or acceleration of repair are unknown in humans. Temporary destruction of epidermal nerve fibers by shock waves also has been observed in animal studies and considered a possible ex- planation for the immediate effects of ESWT. Again, no comparable human study has been performed. Lee et al applied ESWT to treat 435 patients with chronic fasciitis, including 283 heels with inferior calcaneal bone spurs. The results failed to show a correlation between the pres- ence or absence of the heel spur and the 1-year treatment outcome. Hammer et al9 reported the thickness of the plan- tar fascia was substantially reduced among patients who reported less pain at 6 months followup. Nevertheless, the study did not adjust for other confounding variables.
We hypothesized the improvement of pain observed in patients with chronic plantar fasciitis was associated with the reduction of plantar fascia thickness after ESWT. We also asked whether various demographic factors (gender, age, job, exercise habits, body height, body weight, body mass index, employment or not, prior steroid injection, plantar fascia thickness, low- or high-intensity treatment, other treatment during followup) predicted pain improve- ment and association between changes in pain and plantar fascia thickness.

MATERIALS AND METHODS
We prospectively recruited volunteers from our outpatient clin- ics. All patients were diagnosed with plantar fasciitis by certified orthopaedists or physiatrists. The diagnosis was based on history (heel pain, morning pain) and clinical examination (presence of tenderness over the medial tuberosity of the calcaneus) and was reconfirmed by one author (HWL). We included patients with pain lasting at least 6 months and with unsatisfactory results of one or more treatments (medication, orthotics, local steroid in- jection, physical therapy). Patients who had received prior local steroid injection were not excluded from the study, but at least 3 months was required from injection to first ESWT. The patients excluded were those younger than 18 years or those with neu- rologic disorders, sciatica, local infections, local tumors, coagu- lation disorders, or pregnancy. The study was approved by the ethics committee of National Taiwan University Hospital. All patients provided informed consent before treatment.
All the eligible subjects answered a questionnaire to provide demographic data (age, gender, body height, body weight, em- ployment, exercise habits) and treatment received before enroll- ment. The estimated sample size was 33 subjects for each group to test a 30% difference with an level of 0.05 and 80% power. Fifty-three subjects with 78 symptomatic feet were enrolled dur- ing the study period. The patients were randomly assigned to either the group receiving high-intensity treatment (28 of 53 [52.8%]) or the group receiving low-intensity treatment (25 of 53 [47.2%]). The randomization was performed by an independent, blind observer. Binary random numbers were generated by computer software and then sealed. The seals were opened only before the ESWT to decide the intensity of treatment. The sub- jects included 37 women and 16 men with an average age of 50 years (standard deviation,11 years; range, 27–78 years) (Table1). The average body mass index was 25 kg/m2 (standard devia- tion, 4 kg/m2; range, 20–39 kg/m2). Two-thirds of the subjects were employed and 23% of all subjects reported exercising regu- larly. Twenty-five of the 53 patients (47%) had bilateral symp- toms, and all received at least one kind of nonESWT treatment before this study; wearing orthotic footwear was the most com- mon treatment (77%). Twenty-three feet (including 19 treated feet) received steroid injections. The demographic data, includ- ing age, gender, exercise habits, body mass index, and employ- ment rate, were similar between the low- and high-intensity groups (Table 1).
Extracorporeal shock wave therapy was performed with Pi- ezoson 100 (Richard Wolf, Knittlingen, Germany). This is a piezoelectric-type device with an energy flux density ranging from 0.1 to 1.95 mJ/mm2 divided into 20 energy levels. The patients in the low-intensity group received 0.12 mJ/mm2 and those in the high-intensity group received 0.56 mJ/mm2; both groups received three sessions of ESWT (2000 shock waves per session) at weekly intervals. No local anesthesia was applied during treatment. This instrument was not accompanied by in- line ultrasound, and the target of treatment was determined by the self-reported tender site and a sonographic examination be- fore ESWT. We used the approach suggested by Ogden et al15 to apply the shock waves to the maximum pain sites and to the surrounding area within a 1-cm radius. All patients tolerated the treatment intensity, and no ecchymosis or other important ad- verse effect was observed during followup.
Outcome evaluation included a questionnaire and ultrasono- graphic measurement of plantar fascia thickness before ESWT and at followup (3 and 6 months after completion of ESWT).

The questionnaire included average pain severity in the past 1 week (a 10-cm unscaled visual analog scale [VAS] with 0 no pain, 100 extreme pain), the Taiwan Chinese version of the Foot Function Index,2 and the Taiwan Chinese version of the Short Form-36 Health Survey (SF-36).5 Improvement was rated with a 6-point Likert scale with 1 cured, 2 greatly im- proved, 3 moderately improved, 4 mildly improved, 5 not improved, and 6 worse. Pain severity and improvement were rated for each foot. The subjects were asked to discontinue other treatment as possible, and we recorded any other treatment they received during the followup. Treatment was considered successful when the foot pain was rated as cured or greatly improved on the 6-point Likert scale or had a VAS score less than 10. All subjects completed three sessions of ESWT, but one subject in the low-intensity group was lost to followup at 6 months.
Measurement of the plantar fascia thickness was performed by one of the authors (WSC) with a portable ultrasound (Titan; SonoSite Inc, Bothell, WA) and a 10-MHz linear probe on the same day before the first ESWT and at the 3- and 6-month followup. The examiner was blind to the treatment condition. The subjects were examined in the prone position with the knee in full extension and the feet hanging over the edge of the ex- amination bed.28 The probe of the ultrasound was placed on a line connecting the second toe and the midheel. The thickness of the plantar fascia was determined at its proximal end close to insertion into the calcaneus by longitudinal sonograms of the heel. An adequate amount of jelly was applied to eliminate com- pression on the skin by the transducer. A pilot study of 14 patients (eight women and six men; average age, 37 ± 13 years) was used to evaluate the test-retest reliability of the measure- ment. The results revealed the intraclass correlation coefficient of these measurements to be 0.9 (95% confidence interval, 0.7–0.97; p < 0.001).
All descriptive data were expressed as means or proportions as indicated. Analysis was performed by SAS System for Mi- crosoft Windows (SAS 9.1; SAS Institute Inc, Cary, NC). First, a paired t test was used to compare the changes in pain as assessed by the VAS, plantar fascia thickness, Foot Function Index scores, and SF-36 scores before and after treatment to show the effect of ESWT. The differences in characteristics between feet treated successfully and unsuccessfully were com- pared with an independent t test or chi square test. To explore the effect of plantar fascia thickness on the self-reported pain, we conducted multiple marginal linear regression analysis using the stepwise variable selection method. Because the self-reported pain was measured repeatedly over time, the generalized esti- mating equations method for longitudinal data was applied to adjust the standard errors of the regression coefficient estimates using the REPEAT model option of the GENMOD procedure in the SAS software. The independent variables considered in the regression analysis were personal characters (gender, age, job, exercise habits, body height, body weight, body mass index, employment or not) and treatment-related factors (prior steroid injection, plantar fascia thickness, low- or high-intensity treat- ment, other treatment during followup). The patients who were lost to followup or who received other treatment during followup were not excluded from the regression analysis, but the extra treatment was included as an independent variable in the regres- sion model. The interactions between followups and ESWT in- tensity, other treatment received, and plantar fascia thickness also were examined in the model. A p value less than 0.05 was considered statistically significant.
RESULTS
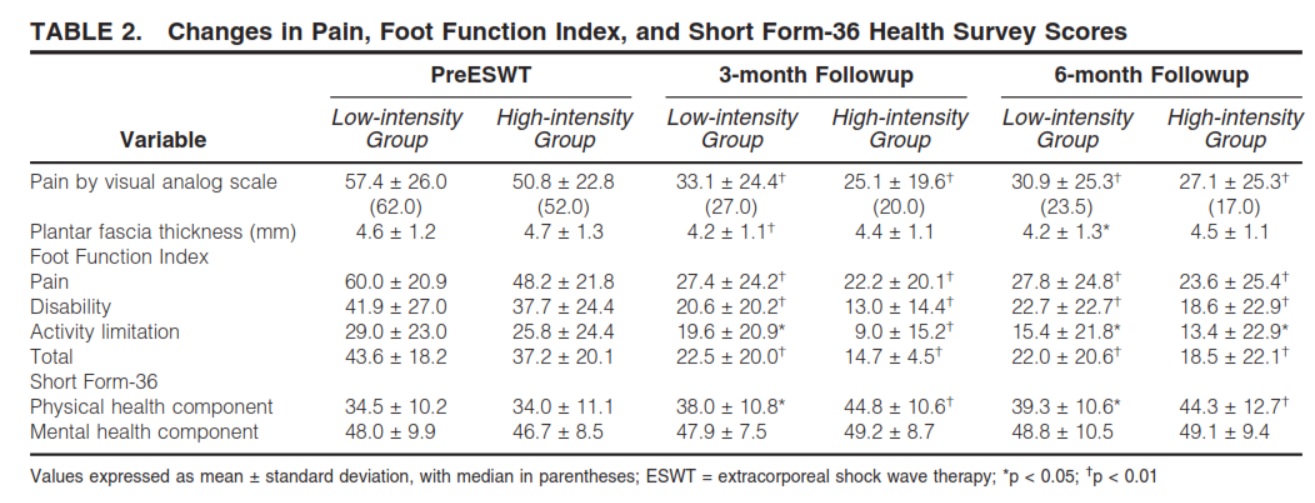
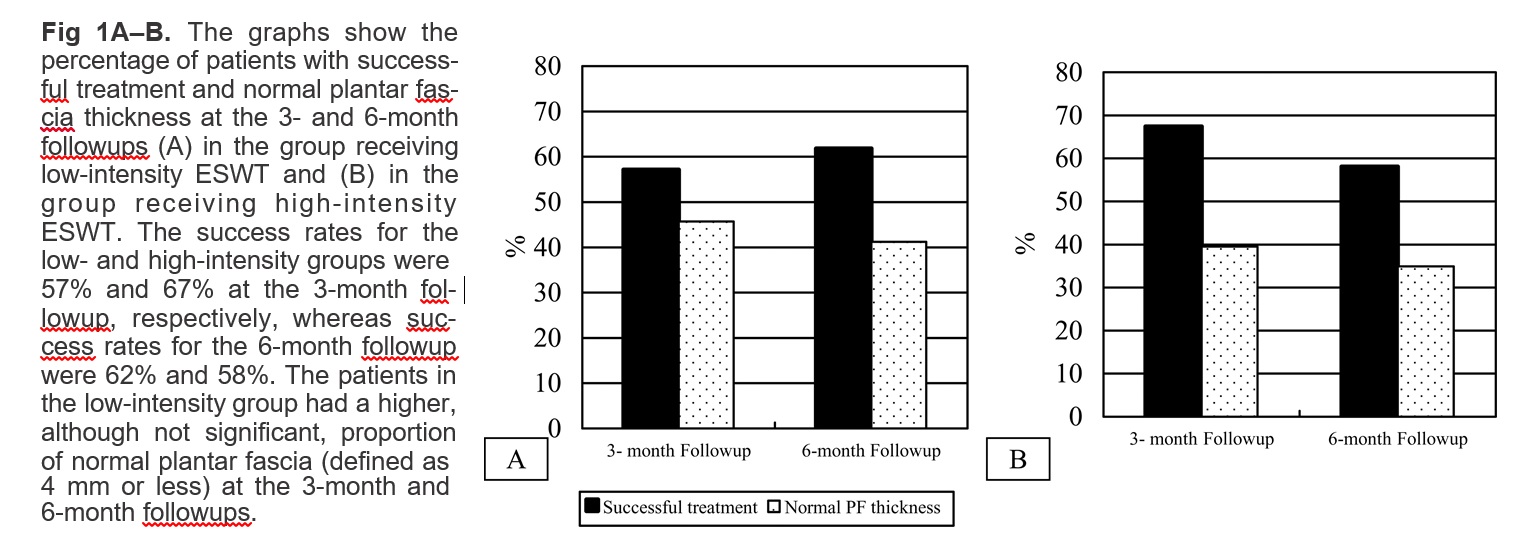
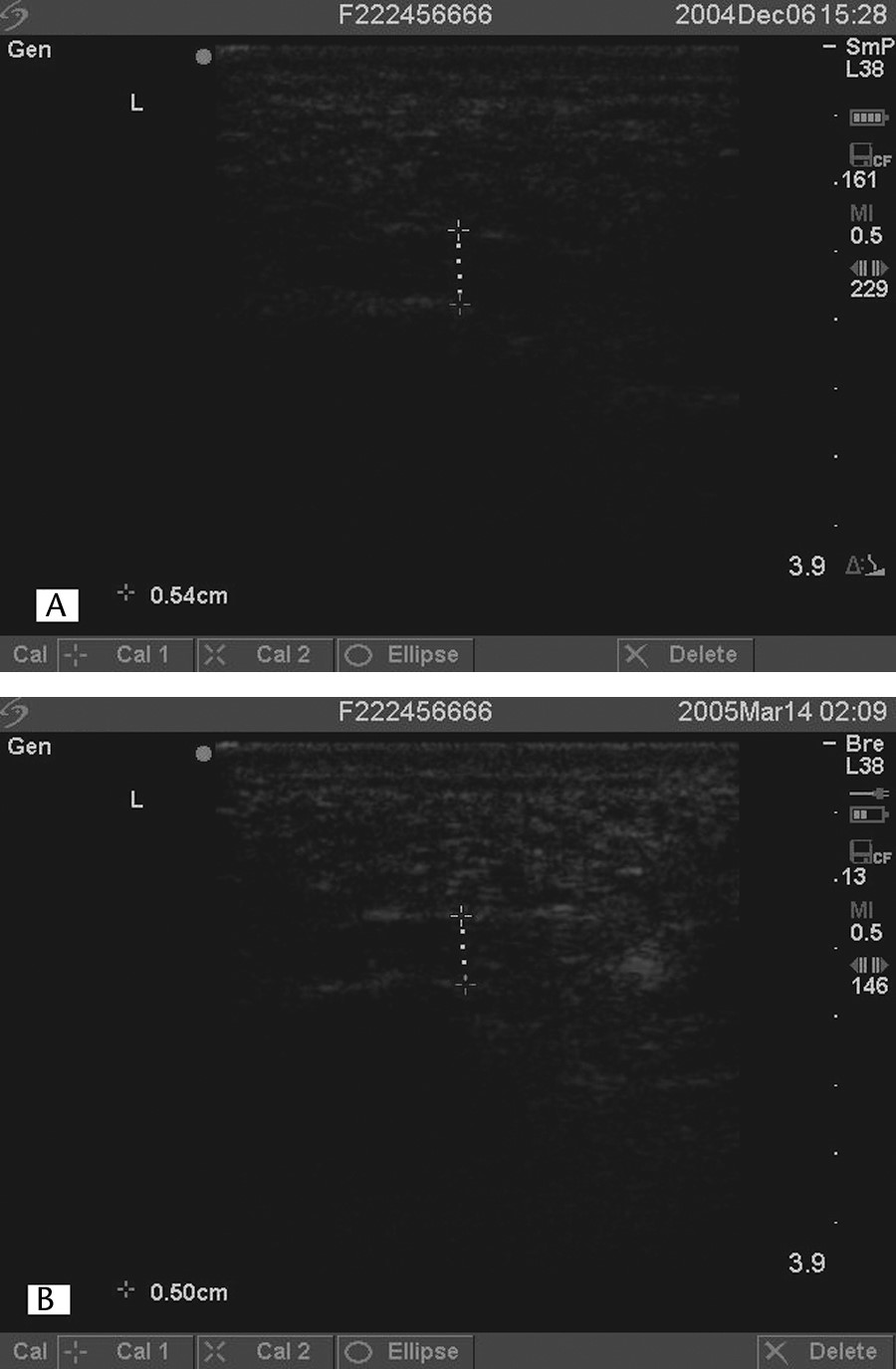
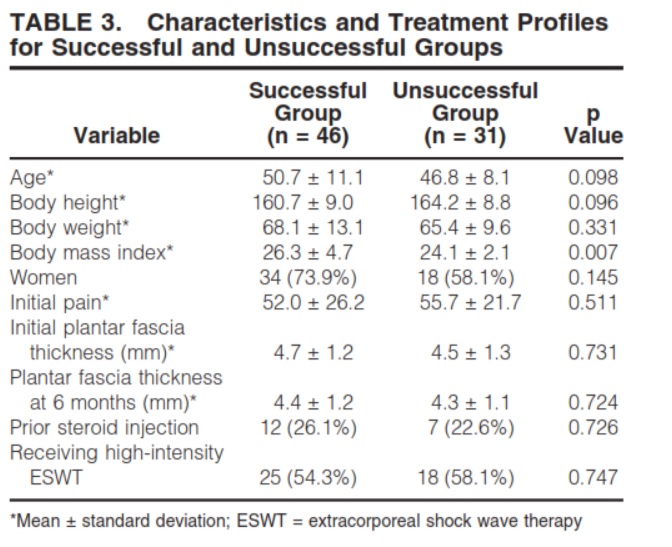
Pain levels, total score, and subscores of the Foot Function Index and the physical health component of the SF-36 were improved at the 3-month and 6-month followup (Table 2). Pain in the patients in the low-intensity group was reduced (p < 0.01) from 57 ± 26 (median, 62) to 31 ± 25 (median, 24), whereas pain in the patients in the high- intensity group was reduced (p < 0.01) from 51 ± 23 (median, 52) to 27 ± 25 (median, 17). At the 3- and 6-month followups, the proportion of patients achieving greater than 50% pain reduction was 46% and 51%, respectively, for all treated feet. The overall successful treat- ment rates were 63% and 60% at the 3- and 6-month followups, respectively. For the low-intensity group, the success rate was 57% at the 3-month followup and 62% at the 6-month followup, whereas the success rates for the high-intensity group were 67% and 58%, respectively (Fig 1). The proportion of normal plantar fascia (defined as 4 mm or less) also was similar between the two groups on two followup occasions. Some patients had thinner but still abnormal plantar fascia thickness (Fig 2). Forty-one percent of the low-intensity group and 35% of the high- intensity group had normal plantar fascia thickness. The characteristics of successfully and unsuccessfully treated feet were mostly similar (Table 3), except that patients with successfully treated feet had a higher body mass in- dex (26 versus 24 kg/m2; p 0.007). Plantar fascia thickness, time of followup, body mass index, ESWT intensity, receiving other treatment during followup, and exercising regularly predicted self-reported pain. The mean level of the self-reported pain level was lower (p < 0.0001) at the 3-month and 6-month followups,
but the effect estimates ( ˆ 1 −26 and ˆ 2 −27) were similar on these two occasions (Table 4). Lower pain levels were associated with thinner plantar fascia thickness (p 0.006), receiving high-intensity ESWT (p 0.03), and exercising regularly (p 0.008). Although the pa- tients in the successfully treated group had a higher body mass index, it was not associated with the mean level of self-reported pain in the multiple marginal linear regres- sion analysis after adjusting for the effects of the other covariates in the regression model.
DISCUSSION
Extracorporeal shock wave therapy has been used for a decade to treat plantar fasciitis, but the underlying treatment mechanism is not well understood. Increased thick- ness of plantar fascia is common among patients with plantar fasciitis, and previous studies have shown reduction of the thickness after ESWT or steroid injection.6,9,29 We hypothesized a decrease of plantar fascia thickness was associated with pain reduction for plantar fasciitis patients after ESWT. One limitation of our study is there was no untreated control group and a placebo effect or natural recovery could not be totally ruled out. There are several ways to assign a sham treatment, such as using the lowest inten- sity or a low dose, aiming the beam elsewhere, or apply- ing a Styrofoam block.1,15 Because our interest was in the correlation between pain and echographic find- ings, such sham or untreated results would be unrepre- sentative of treated patients. Another limitation is that our ESWT was not guided by in-line ultrasound or fluoros- copy, and the imprecision of treatment might be con- sidered one reason for the lack of response to treatment. In contrast to calcified tendinitis of the rotator cuff, the plantar fascia is easily approached and localized using a portable ultrasound. Such additional precision might in- fluence the treatment effect but should be a random ef- fect for measurement of plantar fascia thickness. A final limitation is that we limited followup to a maximum of 6 months, which might be a reason we were unable to observe a more substantial change in plantar fascia thick- ness.
At the 3- and 6-month followups, patients with chronic plantar fasciitis after ESWT showed improvement in pain and foot function. The data supported the hypothesis that pain level was positively associated with plantar fascia thickness. Also, receiving high-intensity ESWT and exer- cising regularly were associated with less pain. Some of these findings had not been observed before and further discussion is warranted.
Thickening of the plantar fascia in plantar fasciitis has been documented in several studies.6,18,24,28 Most studies reported an average thickness greater than 5 mm in the painful plantar fascia, slightly higher than that found in our study (4.6 mm). Steroid injection substantially reduces the thickness, as much as 1.5 mm.6,29 This change could be observed as soon as 2 to 4 weeks after injection. Genc et al6 also found a correlation between pain reduction and plantar fascia thickness. A similar effect of ESWT on plantar fascia thickness was reported by Hammer et al,9
but the decrement was less obvious (5.2 mm to 4.4 mm at the 24-week followup) than that observed in patients re- ceiving steroid injections. The reduction was stable be- tween 6 and 24 weeks after treatment. Our study showed a smaller reduction only in feet receiving low-intensity ESWT (4.6 mm to 4.2 mm). We attributed this to the relatively high proportion (24%) of prior steroid injec- tions; those cases were excluded in the aforementioned
studies. We were careful to require a 3-month interval between steroid injection and first ESWT, which meant the first followup was at least 6 months after steroid in- jection. We also included prior steroid injection as a con- founder in the multiple marginal linear regression model. Therefore, we do not consider the reduction of pain or plantar fascia thickness to be the result of the steroid in- jection. In contrast to the absence of a correlation between the heel spur change and pain improvement after ESWT,13
we observed a positive association between pain level and plantar fascia in our multiple marginal linear regression model. We suggest thickening of the plantar fascia is of pathologic origin and partially parallels symptoms.
We found two additional factors (receiving high- intensity ESWT and exercising regularly at baseline evaluation) associated with lower pain levels in our multiple marginal linear regression model. The intensity or the de- livered energy is considered a key factor for successful treatment by some researchers and is determined primarily by the types of generators and the levels of intensity. There are three shock wave generation methods, including elec- trohydraulic, electromagnetic, and piezoelectric types. Each is characterized by a different intensity of sound pressure, size of focus area, and overall volume of the applied shock waves.3,16 The piezoelectric-type generator has relatively high intensity per focal area but has the smallest focal area, so its total energy is lower.3 Stimula- tion by the piezoelectric lithotriptor is reported to be less painful than stimulation by the other types of generators,25
and most patients can tolerate the treatment without local anesthesia. Our success rate, 60% at 6 months, was within the range reported in previous studies (41–77%). However, whether the lower total energy level results in a different treatment efficacy requires more research.
Energy level is another factor influencing the energy delivered. Although there is some debate regarding the definition of low-intensity treatment, our selected levels of shock wave intensity, 0.12 and 0.56 mJ/mm2, were not different from previously recognized levels for low and high intensities.15,22,23 High-energy (0.32 mJ/mm2) ESWT appeared superior to low-energy (0.08 mJ/mm2) ESWT in treating chronic calcifying tendinitis of the shoulder,7 but no similar results were reported for plantar fasciitis. Nev- ertheless, an animal study showed high-energy electro- magnetic ESWT induced inflammatory changes in the ten- dons and paratendons, and the researchers suggested high- energy ESWT should be avoided.21 In our study, the feet receiving high-intensity ESWT had an approximate nine- unit decrease in the mean level of self-reported pain in our multiple marginal linear regression analysis, but the per- centages of successful treatment were similar for the two groups. For the low-intensity group, the rates were 57% and 62% at the 3- and 6-month followups, respectively, and for the high-intensity group, the rates were 67% and 58%, respectively (Fig 1). The high-intensity group had a higher rate of success at the 3-month followup but a lower rate at the 6-month followup. Extracorporeal shock wave therapy could cause sensory nerve destruction, and a cu- mulative effect might delay regeneration as much as 6 weeks.27 This may be responsible for the short-term pain relief, and a dose-response relationship related to intensity also might exist. Although no apparent adverse effects were observed in our patients, we do not suggest the regu- lar therapeutic use of high-intensity ESWT, given the ab- sence of a superior overall success rate and the risk of potentially adverse effects.
We also observed regular exercise (three times or moreper week) had a favorable outcome in terms of pain level. We could not explain the findings further because no more information about exercise habits was collected during the followup period. Stretching exercise has proved beneficial for patients with plantar fasciitis.4 Details regarding the habits of general exercise and the use of plantar fascia- specific stretching exercise, should be collected to clarify the effects of exercise on pain improvement. Furthermore, the patients in the successfully treated group had a higher body mass index, but it was not significant in our multiple marginal linear regression analysis. Patients with plantar fasciitis have been found to have higher plantar fascia thickness and higher body mass index.24 The temporal relationship between these factors and the symptoms need additional study.
We observed a positive correlation between pain level and plantar fascia thickness after ESWT. Ultrasonographic findings could be a potential indicator of symptoms. The patients in the low- and high-intensity groups showed sub- stantial improvement in terms of pain and function after ESWT. Receiving high-intensity ESWT, although associ- ated with lower pain, did not result in a higher success rate at the end of followup. We therefore suggest using low- intensity ESWT because it is not associated with inferior outcome and induces less discomfort during treatment.
Acknowledgments
We thank Dr. Fu-Chang Hu, National Center of Excellence for General Clinical Trial and Research, National Taiwan University Hospital and College of Public Health, for his suggestion of the generalized estimating equations method and Chia-Chi Cheng for assistance in the generalized estimating equations analysis.
References
1. Buchbinder R, Ptasznik R, Gordon J, Buchanan J, Prabaharan V, Forbes A. Ultrasound-guided extracorporeal shock wave therapy for plantar fasciitis: a randomized controlled trial. JAMA. 2002;288:
1364–1372.
2. Budiman-Mak E, Conrad KJ, Roach KE. The Foot Function Index: a measure of foot pain and disability. J Clin Epidemiol. 1991;44: 561–570.
3. Buizza A, Dell’Aquila T, Giribona P, Spagno C. The performance of different pressure pulse generators for extracorporeal lithotripsy: a comparison based on commercial lithotripters for kidney stones. Ultrasound Med Biol. 1995;21:259–272.
4. Digiovanni BF, Nawoczenski DA, Malay DP, Graci PA, Williams TT, Wilding GE, Baumhauer JF. Plantar fascia-specific stretching exercise improves outcomes in patients with chronic plantar fasciitis: a prospective clinical trial with two-year follow-up. J Bone Joint Surg Am. 2006;88:1775–1781.
5. Fuh JL, Wang SJ, Lu SR, Juang KD, Lee SJ. Psychometric evaluation of a Chinese (Taiwanese) version of the SF-36 Health Survey amongst middle-aged women from a rural community. Qual Life Res. 2000;9:675–683.
6. Genc H, Saracoglu M, Nacir B, Erdem HR, Kacar M. Long-term ultrasonographic follow-up of plantar fasciitis patients treated with steroid injection. Joint Bone Spine. 2005;72:61–65.
7. Gerdesmeyer L, Wagenpfeil S, Haake M, Maier M, Loew M, Wortler K, Lampe R, Seil R, Handle G, Gassel S, Rompe JD. Extracorporeal shock wave therapy for the reatment of chronic





