 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Nikola
Nikola Kayser
Kayser Fusion
FusionEvaluation of plantar fasciitis improvement after shock wave therapy
- Type: Free
Evaluation of plantar fasciitis improvement after shock wave therapy in calcaneal spur patients by musculoskeletal ultrasonography
Soad Said El Molla1, Ahmed M. Fahmy2, Amr Mohamed Gamil1, Rehab Ali Ibrahim3* and Mai Mohamed Kamel1
Abstract
Background: Plantar fasciitis due to calcaneal spur is a common cause of heel pain and functional disability, and its management presents a huge challenge for clinicians which results sometimes in unpleasant clinical outcomes. The efficacy of extracorporeal shock wave therapy (ESWT) as an alternative therapeutic option to surgical management after failure of conservative treatment has been addressed. Our aim was to evaluate the efficacy of ESWT in the treatment of plantar fasciitis in calcaneal spur patients using ultrasonography.
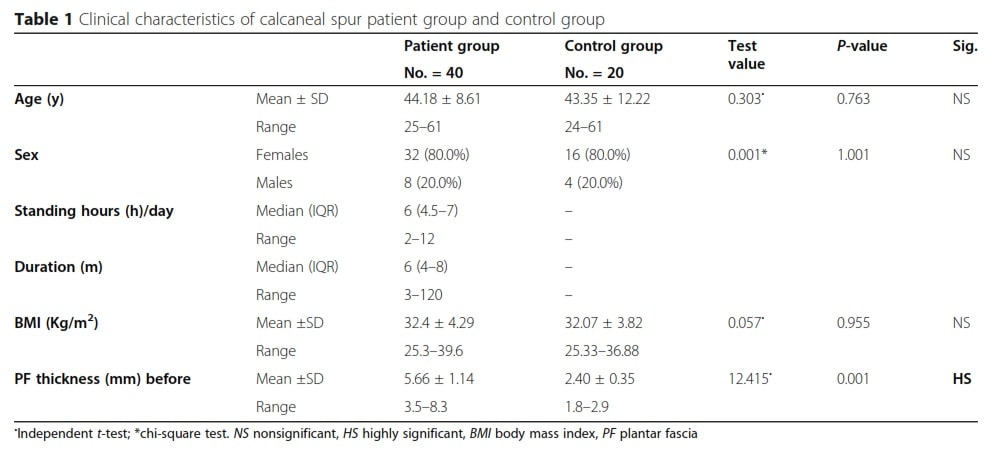
Results: The mean plantar fascia (PF) thickness was statistically significantly higher in the calcaneal spur patient group (5.66 ± 1.14 mm) than in the healthy control group (2.40 ± 0.35 mm), (P = 0.001). Significant PF thickness reduction, visual analog scale (VAS), and Roles and Maudsley score (RMS) improvement were observed (P < 0.001) after 4 sessions of ESWT.
Conclusion: PF thickness increases significantly in calcaneal spur patients and responds to treatment. ESWT decreases the thickness of the PF and improves pain and function significantly.
Keywords: Calcaneal spur, plantar fasciitis, extracorporeal shock wave therapy, Ultrasonography, Heel pain
Background
Calcaneal spur is a chronic condition and is common in adult persons. It can be a cause of plantar fascia (PF) inflammation, leading to restriction of functional activities [1].
Plantar fasciitis is a frequent source of heel pain. It can affect 10% of the population. Plantar fasciitis can result from injury of the PF or due to disturbed biomechanics of the foot [2].
Risk factors include increased body weight, female gen- der, differences in limb length, altered biomechanics of the foot such as pronated foot, and prolonged standing [3].
It is usually a self-limiting condition and 90% of the patients can be treated conservatively using orthotics, no steroidal anti-inflammatory medications (NSAIDs), and exercises [4].
Surgical treatment is reserved for refractory plantar fasciitis, usually after 6–12 months of ineffective treatment. Nevertheless, surgical treatment carries a risk of multiple complications [5].
The use of extracorporeal shock wave therapy (ESWT) has been introduced in the 1990s as a therapeutic option for insertion tendinopathies, as it aids in the healing process. It has been recently used in the treatment of plantar fasciitis which is refractory to the usual conservative measures [6, 7].
The American Food and Drug Association (FDA) approved the use of ESWT in calcaneal spur after the positive results of Ogden et al. [8] and Buch et al. [9].
Ultrasonography has been well documented as a useful noninvasive diagnostic modality for plantar fasciitis [10],
with advantages of being non-invasive, with no risk of radiation, and low cost [11].
Aim of the study
The present study aimed at evaluating the efficacy of shock wave therapy for plantar fasciitis in calcaneal spur patients by musculoskeletal ultrasonography.
Methods
The study included forty patients of both sexes with a planter calcaneal spur confirmed by x ray images attending the outpatient clinic of the National Institute of Neuro Motor System as a patient group and twenty (20) healthy individuals with matched age and sex as control group.
Inclusion criteria
Age > 18
- Symptoms: heel pain > 3 months, unsuccessful conservative treatment > 6 mont
- Pain > 5 by visual analog scale (VAS) and investigator assessm
- Two failed pharmacologic treatments.
- Two failed no pharmacologic treatments.
- Single site of tenderness over plantar calcaneal tuberosity.
No other treatment or drugs (NSAIDs, steroids and other analgesics) were used for 4 weeks before the study began or during the study period.
Exclusion criteria
We excluded patients with:
- Recent significant disease (Inflammatory arthritis, seronegative disease).
- Prior surgery for plantar fasci
- Neuropathy, malignancy, or
- Plantar Fascial
- Bilateral
- Pregnancy.
- Corticosteroid injection within 6 wee
- Physical therapy within 2
- Narcotic
- NSAIDS within 48 h
- Anticoagulant medication
These patients were submitted to:
- Full history taking, general clinical examination, and local examination of the foot.
- Weekly ESWT sessions. An ESWT device with an electrohydraulic system of (Orthospec, Medispec Inc, Montgomery Village, MD, USA) with a fixed Focus of 25 × 95 mm was used. Every patient received 4 consecutive sessions (once a week) with1000 shocks at a frequency of 96 shocks per minute. The energy density was 0.077 mj/mm2and gradually increased to 0.32 mj/mm2 to avoid initial treatment pain. The energy was dispersed over a treatment area that was large enough that the intensity of the shockwaves reached therapeutic levels while remaining generally well tolerated by recipient patients without the need for anesthesia or sedation. The effective distribution of the shockwaves is over a broad enough anatomical area that there is no need for ultrasonic or radiographic targeting.
- Blinded to the clinical data, musculoskeletal ultrasound imaging was conducted using 18/7 MHz linear array transducer (Toshiba, Aplio 400, Japan) to evaluate PF thickness in millimeters is about 2 cm distal to the medial calcaneal tuberosity [12]. Pre-ESWT and after 8 weeks. Participants were prone with toes resting upon the examination table. The fascia was traced in longitudinal and transverse planes from the level of the calcaneal attachment to the forefoot using B mode. Adjustment of the pain and focal point was done as necessary to optimize the image. The presence of calcification/echogenic foci within the fascia, fibers interpretation, and edema of heel fat pad were recorded.
- The degree of pain felt by the patients was measured subjectively using a VAS ranging from 0 = no pain to 10 = maximum pain. The Roles and Maudsley score (RMS) was used as a functional evaluation method in four level grading categories (excellent 1 indicates no pain, full movement, and activity; good 2 indicates occasional discomfort, full movement, and activity; fair 3 indicates some discomfort after prolonged activity; and poor 4 indicates pain-limiting activities), based on pain and activity ranges in daily life in pre-ESWT and after 8 weeks [13].
X-ray was one for the control group to exclude calcaneal spur and musculoskeletal ultrasound for measurement of PF thickness.
Statistical analysis
Data were collected and entered into the statistical Package for Social Science (IBM SPSS) version
- The quantitative data were explored for distribution using Kolmogorov-Smirnov and presented as means, standard deviations, and ranges for parametric variables and median with interquartile range (IQR) for non- parametric variables. Also, qualitative variables were presented as numbers and percentages. The comparison between two independent groups with quantitative data and parametric distribution was done using the independent t-test while non-parametric data were done by using the Mann-Whitney test. The confidence interval was set to 95% and the margin of error accepted was set to 5%. So, the P-value was considered significant at the level of ≤ 0.05. Correlation between variables was done using Pearson’s correlation test.
Ethical consideration
Approval of the study conduction was obtained from the ethical committee. Written informed consent was obtained from all participants.
Results
The study included forty calcaneal spur patients attending the physical medicine, rheumatology, and rehabilitation outpatient clinic.
The selection was from both sexes; they were 32 females (80%) and 8 males (20%). Their age was 44.18 ±8.61 (range: 25–61 years). Their body mass index (BMI) was 32.14 ± 4.35 (range: 25.3–39.6 Kg/m2), 12 over- weight (27.5%), and 28 obese (72.5%). Their disease duration ranged between 3 and 120 months with a median (IQR) of 6 (4-8).
They were compared to 20 normal control subjects, 16 female (80%) and 4 male (20%). Their age was 43.35 ±12.2 (range: 24–61years). There was no significant difference in age, sex, and BMI between the two groups(Table 1).
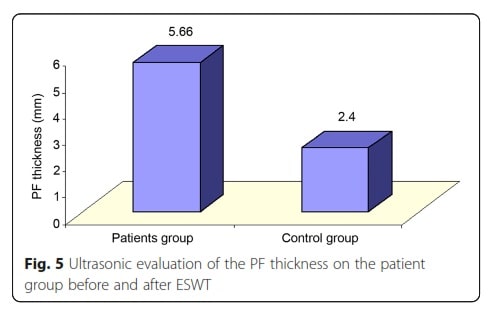
Pain and functional affection were the presenting features of our patients, (100%) with VAS median (IQR) 8 (7–8) and Roles and Maudsley median (IQR) 4 (4–4).On ultrasound examination before ESWT, 40 (100%) of the patient group showed increased PF thickness which was significantly (P = 0.001) greater in the calcaneal spur patients (5.66 ± 1.14 mm) than in the asymptomatic control individuals (2.40 ± 0.35 mm) (Table 1). Thirty-eight (95%) of the patients showed abnormal focal low echogenicity in the PF, 30 (75%) perifascial edema, and 2 (5%) calcifications.
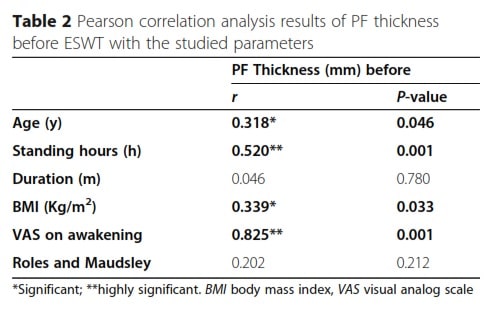
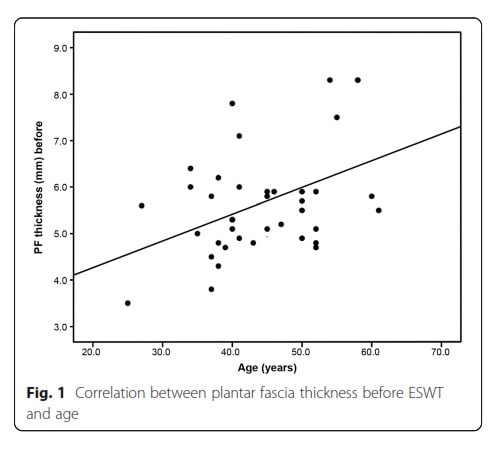
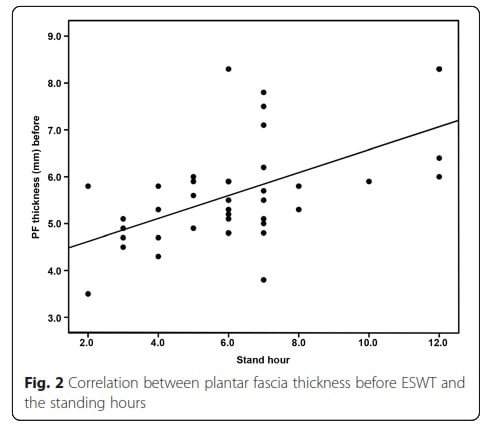
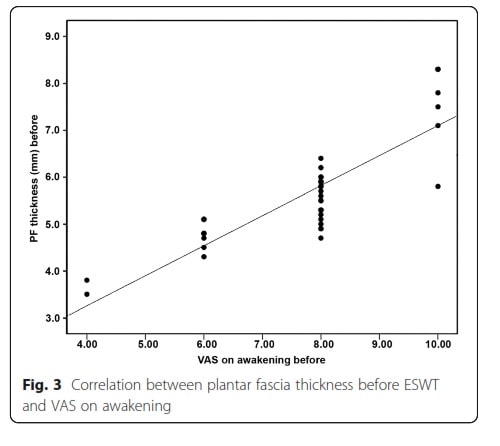
There was a strong positive significant correlation be- tween PF thickness before ESWT and the age (P ≤ 0.05), standing hours (P = 0.001), BMI (P ≤ 0.05), and VAS on awakening (P = 0.001) (Table 2) (Figs. 1, 2, and 3).
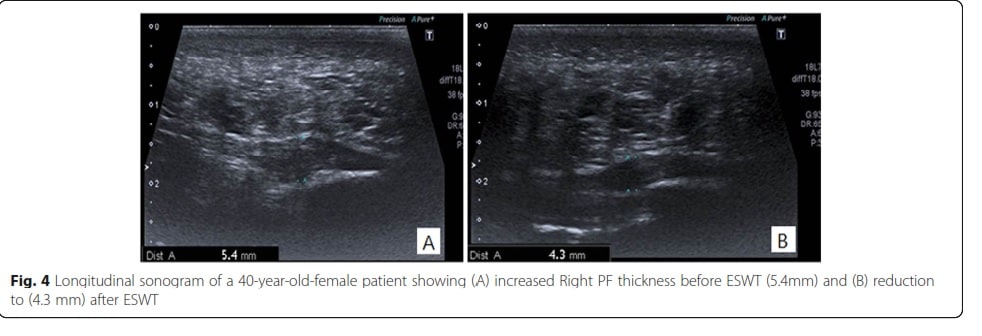
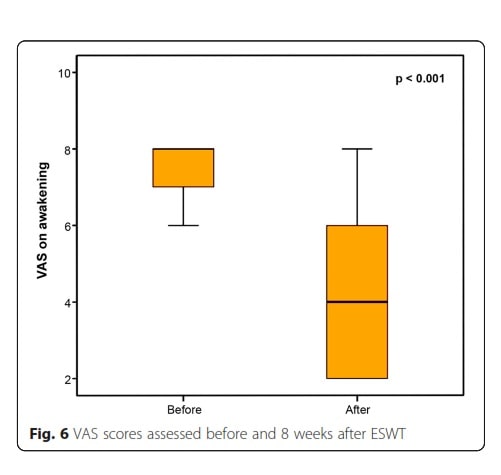
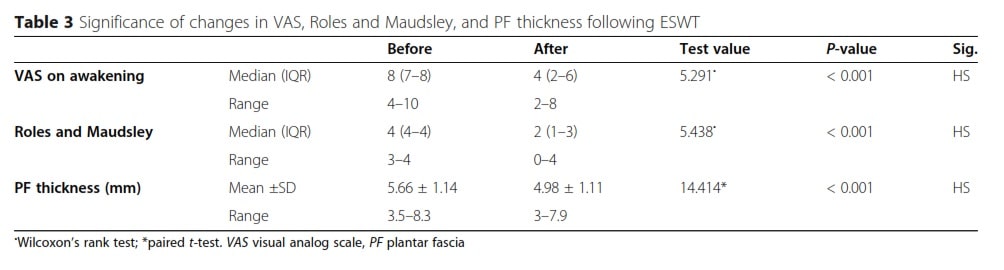
Eight weeks after ESWT, the decrease in PF thickness in calcaneal spur patients (5.66 ± 1.14 to 4.98 ± 1.11 mm) was highly significant (P < 0.001) (Figs. 4 and 5). A highly significant decrease of median values of VAS from
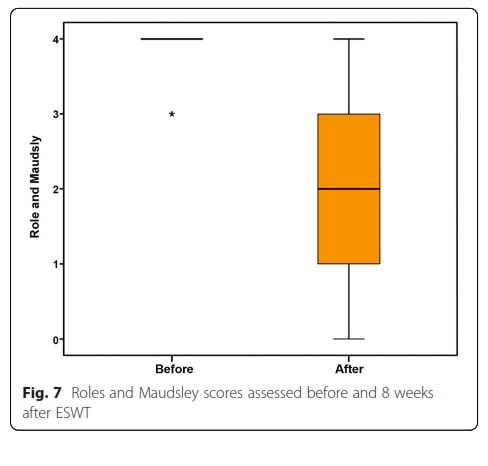
8 to 4 (Fig. 6) and Roles and Maudsley score from 4 to 2 (P < 0.001) (Fig. 7) was seen 8 weeks after the end of ESWT (Table 3).
No statistically significant correlation between the reduction of PF thickness and decrease in pain and functional scores was demonstrated (Table 4).
Discussion
The PF is a group of elastic and collagenous fibers which originates from the medial part of the calcaneus and is attached to the forefoot along with various other tissues. Under the effect of chronic strain, elastic fibers become straight and stiffening of the fascia occurs [14].
Plantar heel pain can be linked to calcaneal spur, a condition that affects many people of all ages. It is a bony outgrowth on the heel bone. The spur tip site is within the PF origin leading to persistent traction on the PF and triggering its inflammation [15]. Calcaneal spur can be symptomatic especially with aging, obesity, in female patients, and in patients with history of osteoarthritis [16].
It is usually a self-limiting condition. Most of the patients’ symptoms are relieved by conservative treatments such as corticosteroid injection, NSAIDS, rest, and using orthotics [17]. Sometimes, therapeutic modalities can be used such as therapeutic ultra- sound [18].
There is an agreement that about 90% of heel pain improve with conservative measures and that surgical management can be considered after failure of these non- operative measures. It was reported that ESWT might be a good alternative to surgical maneuvers which might carry the risk of complications [19].
ESWT has been used recently as a noninvasive and effective modality in the treatment of patients with chronic heel pain who are resistant to other com- monly used conservative treatments [8]. FDA ap- proved ESWT as a non-surgical treatment technique in patients with symptomatic plantar fasciitis, who are resistant to other commonly used conservative treat- ments [20]. Also, the FDA approved its use in 2002 in patients with symptomatic heel spurs after the positive results of Buch et al. [8].
Ultrasonography is an important tool in the diagnosis and evaluation of patients with plantar fasciitis through the detection of thickening of the PF and its hypoecho- genic pattern at calcaneal insertion [21].
There might be a debate regarding the clinical out- come of using ESWT as a therapeutic option in the treatment of symptomatic calcaneal spur [22, 23].
Our aim was to evaluate the efficacy of ESWT for plantar fasciitis in calcaneal spur patients by musculo- skeletal ultrasonography.
In the present study, patients were more frequently females (80%), mostly obese, their mean BMI was
32.4 ± 4.29, and their mean duration was 44.18 ±
8.61 years which was in accordance with the results of previous studies which reported that the risk of plantar fasciitis is linked to increased BMI [24]. Patients in the present study had prolonged standing hours with a mean of 6 h, thus indicating the import- ance of mechanical factors in this disease and sup- porting the results of other studies which concluded that plantar fasciitis might be associated with behaviors and occupations related to weight bearing and in- creased standing [25].
The thickness of PF was measured by ultrasound 2 cm distal to the calcaneal tuberosity. In addition, the Level of pain was recorded in the VAS scale and RMS was used as a functional evaluation method. A thick- ness of the PF more than 4 mm is indicative of plantar fasciitis [26]. In our study, a mean PF thickness in calcaneal spur patients (5.66 ± 1.14 mm) was significantly greater than in the asymptomatic control individuals (2.40 ± 0.35 mm).
The main targets of therapies in plantar fasciitis are to decrease the level of pain and increase the level of function. In the present study, we detected high statistical significance regarding pain degree and functional evaluation in plantar fasciitis before and after ESWT treatment P < 0.001), supporting the results of previous studies including Cheing and Chang in 2007 [27] and Ulusoy et al. in 2017 [28].
In 2013, a meta-analysis study reported a decrease in the pain and RMS on using ESWT compared to placebo in contrast to other studies which concluded that ESWT is ineffective in the treatment of plantar fasciitis [2], indicating that assessment of the role and the efficacy of ESWT must be continued as long as there is controversy to detect a conclusive response regarding the target disorder.
Measuring PF thickness can give an idea regarding the effect of the therapeutic device used. According to our study, there was a significant decrease in the thickness of the PF before and after treatment suggesting that it might be used as an objective tool in the follow-up of plantar fasciitis treatment using ESWT.
This study found that the PF thickness was strongly correlated with the number of standing hours and BMI, which might suggest that decreasing the number of Standing hours and reducing body weight might prevent the development of plantar fasciitis; further studies should be done to investigate this finding.
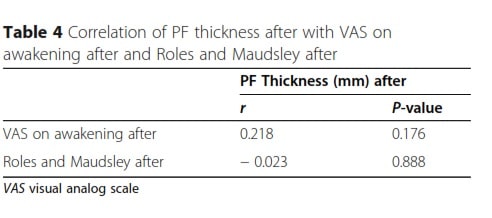
There was no statistically significant correlation between clinical data (VAS and RMS) and PF thickness after ESWT; this might be due to the short duration of the follow-up. Further studies with a longer duration of follow-up are recommended which might reveal the as- association between reduction in PF thickness and clinical data as pain and functional scores.
Limitations
Our study had some limitations. First, short duration of follow-up (8 weeks). Follow-up of extended duration could demonstrate the long-term outcomes of ESWT in patients with symptomatic calcaneal spur. Second, limited sample size. Further studies with a larger sample size are recommended.
Conclusions
We conclude that ESWT is an effective treatment for chronic plantar fasciitis in calcaneal spur patients with significant improvement in pain and function scores. Ultrasound is an important tool in monitoring plantar fasciitis improvement following ESWT.
A prophylactic program including weight reduction and lifestyle modification such as reducing the standing hours is recommended.
Author details
1National Institute of Neuro-Motor System, Giza, Egypt. 2Al-Azhar University, Cairo, Egypt. 3Faculty of medicine, Ain Shams University, Cairo, Egypt. Received: 15 June 2021 Accepted: 6 September 2021
References
- Lizis P, Kobza W, Manko G, Para B, Jaszczur-Nowicki J, Perlinski J (2017) Extracorporeal shock wave therapy and ultrasound waves effectively reduce. symptoms of chronic calcaneal spur. Clin Res Foot Ankle 5:2
- Haake M, Buch M, Schoellner C, Goebel F, Vogel M, Mueller I, Hausdorf, Karin Zamzow J, Schade-Brittinger C, Mueller H (2003) Extracorporeal shock wave therapy for plantar fasciitis: randomised controlled multicentre trial. BMJ 327(7406):75–70. https://doi.org/10.1136/bmj.327.7406.75
- Tahririan MA, Motififard M, Tahmasebi MN, Siavashi B (2012) Plantar fasciitis. J Res Med Sci 17(8):799–804
- Lemont H, Ammirati KM (2003) Usen N (2003) Plantar fasciitis: a degenerative process (fasciosis) without inflammation. J Am Podiatr Med Assoc 93(3):234–237. https://doi.org/10.7547/87507315-93-3-234
- Samuel WYC, Chester LWH, Terence PCT, Lam YHR (2015) The effect of low dose extracorporeal shock wave therapy (ESWT) on plantar fasciitis: a trial study in Queen Mary Hospital. J Orthop Trauma Rehabil 19(2):60–65. https:// doi.org/10.1016/j.jotr.2014.10.005
- Rompe JD, Eysel P, Hopf C, Krischek O, Vogel J, Bürger R, Jage J, Heine J (1997) Extracorporeal shockwave therapy in orthopedics. Positive results in tennis elbow and tendinosis calcarea of the shoulder. Fortschr Med 115(26): 29–33
- Krischek O, Rompe JD, Herbsthofer B, Nafe B (1998) Symptomatic low- energy shockwave therapy in heel pain and radiologically detected plantar heel spur. Z Orthop Ihre Grenzgeb 136(2):169–174. https://doi.org/10.1055/ s-2008-1051301
- Ogden JA, Alvarez R, Levitt R, Cross GL, Marlow M (2001) Shock wave therapy for chronic proximal plantar fasciitis. Clin Orthop 387:47–59. https://
doi.org/10.1097/00003086-200106000-00007
- Buch M, Knorr U, Fleming L, Theodore G, Amendola A, Bachmann C, Zingas C, Siebert WE (2002) Extracorporeal shockwave therapy in symptomatic heel spurs. An overview. Orthopade 31(7):637–644. https://doi.org/10.1007/ s00132-002-0323-z
- McNally EG, Shetty S (2010) Plantar fascia: imaging diagnosis and guided treatment. Semin Musculoskelet Radiol 14(3):334–343. https://doi.org/10.1
- Sabir N, Demirlenk S, Yagei B, Karabulut N, Cubukcu S (2005) Clinical utility of sonography in diagnosing plantar fasciitis. J Ultrasound Med 24(8):1041–
- https://doi.org/10.7863/jum.2005.24.8.1041
- Hammer DS, Adam F, Kreutz A, Rupp S, Kohn D, Seil R (2005) Ultrasonographic evaluation at 6-month follow-up of plantar fasciitis after extracorporeal shock wave therapy. Arch Orthop Trauma Surg 125(1):6–9. https://doi.org/10.1007/s00402-003-0591-z
- Gollwitzer H, Saxena A, DiDomenico LA, Galli L, Bouché RT, Caminear DS, Fullem B, Vester JC, Horn C, Banke IJ, Burgkart R, Gerdesmeyer L (2015) Clinically relevant effectiveness of focused extracorporeal shock wave therapy in the treatment of chronic plantar fasciitis: a randomized, controlled multicenter study. J Bone Joint Surg Am 97(9):701–708. https:// doi.org/10.2106/JBJS.M.01331
- Aquino A, Payne C (1990) Function of the plantar fascia. Foot 9(2):73–78. https://doi.org/10.1054/foot.1999.0520
- Johal KS (2012) Plantar fasciitis and calcaneal spur. Fact or fiction? Foot Ankle Surg 18(1):39–41. https://doi.org/10.1016/j.fas.2011.03.003
- Aldridge T (2004) Diagnosing heel pain in adults. Am Fam Physician 70(2): 332–338
- Tornese D, Mattei E, Lucchesi G, Bandi M, Ricci G, Melegati G (2008) Comparison of two extracorporeal shock wave therapy techniques for the treatment of painful subcalcaneal spur. A randomized controlled study. Clin Rehabil 22(9):780–787. https://doi.org/10.1177/0269215508092819
- Li H, Xiong Y, Zhou W, Liu Y, Liu J, Xue H, Hu L, Panayi AC, Mi B, Liu G (2019) Shock-wave therapy improved outcome with plantar fasciitis: a meta- analysis of randomized controlled trials. Arch Orthop Trauma Surg 139: 1763–1770
- Othman AMA, Ragab EM (2010) Endoscopic plantar fasciotomy versus extracorporeal shock wave therapy for treatment of chronic plantar fasciitis. Arch Orthop Trauma Surg 130(11):1343–1347. https://doi.org/10.1007/s004 02-009-1034-2
- Henney JE (2000) From the food and drug administration: shock wave for heel pain. JAMA 284(21):2711. https://doi.org/10.1001/jama.284.21.2711- JFD00010-2-1
- Karabay N, Toros T, Hurel C (2007) Ultrasonographic evaluation in plantar fasciitis. J Foot Ankle Surg 46(6):442–446. https://doi.org/10.1053/j.jfas.2007.08.006
- Porter MD, Shadbolt B (2005) Intralesional corticosteroid injection versus extracorporeal shock wave therapy for plantar fasciopathy. Clin J Sport Med 15(3):119–124. https://doi.org/10.1097/01.jsm.0000164039.91787.dc
- Saber N, Diab H, Nassar W, Razaak HA (2012) Ultrasound guided local steroid injection versus extracorporeal shockwave therapy in the treatment of plantar fasciitis. Alex J Med 46(1):35–46
- Riddle DL, Pulisic M, Sparrow K (2004) Impact of demographic and impairment-related variables on disability associated with plantar fasciitis. Foot Ankle Int 25(5):311–317. https://doi.org/10.1177/107110070402500506
- Riddle DL, Pulisic M, Pidcoe P, Johnson RE (2003) Risk factors for plantar fasciitis: a matched case-control study. J Bone Joint Surg Am 85(5):872–877. https://doi.org/10.2106/00004623-200305000-00015
- McMillan AM, Landorf KB, Barrett JT, Menz HB, Bird AR (2009) Diagnostic imaging for chronic plantar heel pain: a systematic review and meta- analysis. J foot Ankle Res 2:1
- Cheing G, Chang H (2007) A comparison of the effectiveness of extracorporeal shock wave and ultrasound therapy in the management of heel pain. Shock Waves 17(3):195–201. https://doi.org/10.1007/s00193-007-0102-1
- Ulusoy A, Cerrahoglu L, Orguc S (2017) Magnetic resonance imaging and clinical outcomes of laser therapy, ultrasound therapy, and extracorporeal shock wave therapy for treatment of plantar fasciitis: a randomized controlled trial. J Foot Ankle Surg 56(4):762–767. https://doi.org/10.1053/j.jfa s.2017.02.013





