 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Nikola
Nikola Kayser
Kayser Fusion
FusionEfficacy of Extracorporeal Shock wave Therapy in Frozen Shoulder
- Type: Free
Department of Physical Medicine and Rehabilitation, Isfahan University of Medical Sciences, Alzahra Hospital, Isfahan, Iran, 1Department of Orthopedic Surgery, Isfahan University of Medical Sciences, Alzahra Hospital, Isfahan, Iran
Correspondence to:
Dr. Abolghasem Zare Zade, Department of Orthopedic Surgery, Isfahan University of Medical Sciences, Alzahra Hospital, Soffe Avenue, Isfahan, Iran.
E‑mail: This email address is being protected from spambots. You need JavaScript enabled to view it.
Date of Submission: Sep 22, 2013
Date of Acceptance: Mar 08, 2014
How to cite this article: Vahdatpour B , T ahe ri P =are =aGe $ 0oraGLaQ 6 Efficacy of Extracorporeal S hoc kw ave T he rapy i n F roz e n S houl de r. I nt J P re v M e d 2014 5: 875- 81.
ABSTRACT
Background: Frozen shoulder has always been considered important because of the impact on the quality-of-life and long period of illness. Therefore, the use of noninvasive and safe techniques that can speed up the healing process of the disease is important.
Methods: This study was a randomized clinical trial study on patients suffering from frozen shoulder who were referred to Isfahan University of Medical Sciences hospitals in 2011 and 2012. A total of 36 patients were enrolled in the study. Eligible patients were allocated into two groups. Intervention group received extracorporeal shock wave therapy (ESWT) once a week for 4 weeks. The control group received sham shock wave therapy once a week for 4 weeks. On the follow-up period, changes in individual performance and the amount of pain and disability were assessed by the Shoulder Pain and Disability Index (SPADI) questionnaire and the range of motion changes were assessed by a goniometer. Data obtained were analyzed using SPSS software.
Results: Variance analysis revealed a difference in the mean pain and disability score of the SPADI questionnaire, flexion, extension, and abduction, external rotation of involved shoulder between two groups before and after the shock wave therapy (P < 0.05). Improvement was more satisfactory in the intervention group, but the mean internal rotation did not differ significantly in two groups (P > 0.05).
Conclusions: The use of ESWT seems to have positive effects on treatment, quicker return to daily activities, and quality-of-life improvement on frozen shoulder.
INTRODUCTION
Frozen shoulder is an idiopathic and progressive disease, which is identified by pain and decreased range of motion (ROM) of the shoulder and shoulder joint capsule fibrosis. Adhesive capsulitis occurs in approximately 2-5% of the general population which is 2-4 times more common in women than men, and is most frequently seen in individuals between 40 and 60 years of age the disease is more common in patients with diabetes mellitus, rotator cuff lesions, thyroid disorders, Chronic Obstructive Pulmonary Diseases, cerebrovascular accident, myocardial infarction, inflammatory arthritis, trauma, and prolonged immobilization. Frozen shoulder has many complications such as sleep disturbance, impaired performance in daily activities, and personal grooming. The disease has three phases: In the first phase (pain phase), synovitis, thickening of the joint capsule, synovial fluid loss, and decreased ROM are observed. The duration of this phase is approximately 10-36 weeks. In the second phase (frozen phase), pain is decreased and joint capsule fibrosis, thickening of the rotator cuff tendons, and loss of joint space are seen. The duration of this phase is approximately 4-12 months. In the third phase (resolution phase), joint ROM again increases gradually and the patient gradually returns to normal daily activities. The duration of this phase is approximately 12-42 months. The disease is treatable although treatment is usually long and creates many problems for the patients. Intra-articular corticosteroid injections, physical therapy, supraclavicular nerve block, acupuncture, daily activities modification, etc., are traditionally used in this condition.[1-4] In physical therapy, various modalities such as joint mobilization,[5] heat, transcutaneous electrical nerve stimulation, exercise, distension arthrography and manipulation under anesthesia, arthroscopic and open surgical release are used early in the rehabilitation process; however, passive joint glides and non-painful passive ROM exercises might be beneficial. Early scapular stability exercises and closed chain rotator cuff exercises can be instituted. As the patient’s symptoms improve, active-assisted and active ROM activities can be added, along with open chain and proprioceptive exercises. The Pendulum and University of Washington (Jackins) exercises are useful for improving the shoulder’s ROM.[6-9] Shockwave through generating low-energy waves and electromagnetic excitation could be effective in this condition due to increasing the regional blood flow, neovascular changes, enzymes release, reduction of inflammatory cytokines, and increasing the flexibility of the collagen fibers and tendons in that area. This type of treatment has been used in other orthopedic conditions such as tendinitis,[10-15] plantar fasciitis,[15-17] and lateral epicondilitis[18,19] the healing process of wounds[20] and fractures[21] and satisfactory results have been achieved. There is also limited number of investigations to evaluate the usefulness of shock wave therapy in frozen shoulder. This study aimed to determine the effect of extracorporeal shock wave therapy (ESWT) in the treatment of patients with frozen shoulder admitted to Isfahan University of Medical Sciences hospitals in 2011 and 2012.
METHODS
Study design and participants
This clinical randomized trial study was performed in Kashani Hospital, Isfahan, Iran in 2011 and 2012.
The study population was the patients with frozen shoulder who were admitted to Isfahan Medical University hospital. The patients were examined by a hand surgeon sub-specialist. After providing the necessary X-ray and injection of 40 mg triamcinolone (Hexal AG) into the involved shoulder joint, the patients were referred to the physical medicine and rehabilitation clinic. Exclusion criteria were history of previous surgery on the shoulder, history of shoulder fracture, cancer, inflammatory disorders, bleeding disorders, and unwillingness to participate in the study. Then, the patients completed a consent form to participate in the research. After that, the enrolled patients were randomized into two groups using random allocation software.
Proscure and variable assessment
All the patients received analgesics (meloxicam 15 mg daily), and activity modification to reduce pain, and were advised to perform Pendulum exercises (swinging arm forward and back, side to side, and around in circles for 5-10 times) and stretching the back of the involved shoulder 30 s twice a day. If the patient tolerated it progressed by wall walking and University of Washington (Jackins) exercises, the patients were blind to the study. The patients in the intervention group received shock wave therapy once a week for 4 weeks. The focus probe sets were used and in each session, patients received ESWT from anterior and posterior directions (on the average 1200 shocks between 0.1 and 0.3 mJ/mm2) up to the maximum threshold of pain tolerance in the shoulder. The control group received sham shockwave therapy once a week for 4 weeks while the device was turned off and placed on the patient’s shoulder for the same period of time. The device used in this study was the standard electromagnetic shockwave (Doulith SD1). This procedure was performed with patients in the sitting position on a chair after applying the coupling gel. Pain and disability score were assessed with the Shoulder Pain and Disability Index (SPADI) questionnaire before the treatment, immediately after the intervention, and 2 and 5 months after the intervention. The SPADI questionnaire was completed for each patient by the physician in each session. The SPADI questionnaire’s is a self-administered instrument developed to measure pain (five items) and disability (eight items) associated with shoulder complaints. For the five pain items, “no pain” scored zero and “the worst imaginable pain” scored 10; for the eight disability items, “no difficulty” received zero score while “difficulty requiring assistance” received 10 scores. The SPADI demonstrates good internal consistency, test-retest reliability and criterion and construct validity. It also appears to be able to detect change in patient status over time. The SPADI should therefore prove to be a useful instrument both in clinical practice and in clinical research.[22] The ROM of the involved shoulder was measured by a goniometer in flexion, abduction, extension, internal, and external rotation.
Statistical analyses
The obtained data were analyzed with the Statistical Package for the Social Sciences version 20.0 (SPSS Inc., Chicago, IL, USA), using independent t-test, paired t-test, Chi-square test, and repeated measures ANOVA.
RESULTS
Figure 1 shows a total of 40 patients with frozen shoulder were randomly divided into two groups. The intervention groups received ESWT and the control group received sham ESWT. Four patients
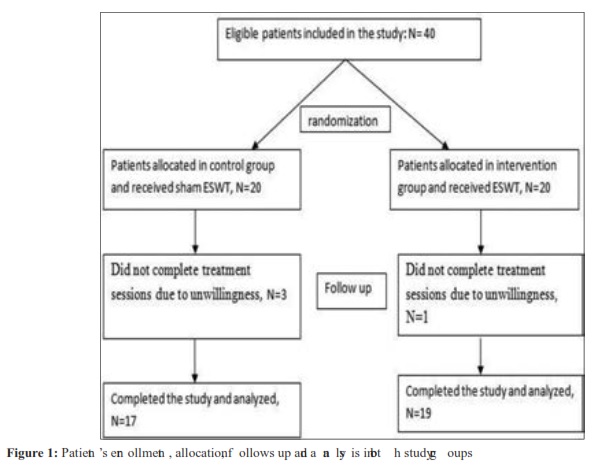
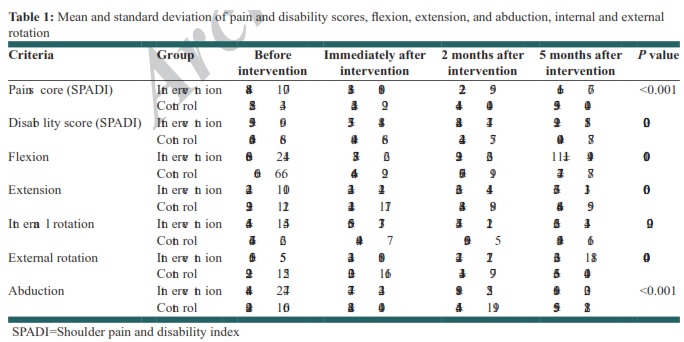
(one in the intervention group and three in the control group) did not complete treatment sessions due to unwillingness; therefore, 19 patients in the intervention group (13 women and 6 men, 68.4% vs. 31.6%) and 17patientsinthe control group(12 women and 5 men, 70.5% vs. 29.5%) completed the study. The mean age of the intervention and control groups was 56.1 ± 10.6 and 60.3 ± 4.8 years respectively and t-test revealed no significant difference between the two groups in this regard (P > 0.05). As for gender distribution in the intervention and control groups, there were 13 females and 6 males. Chi-square test showed no significant difference in gender distribution between the two groups (P > 0.05). Furthermore, the right shoulder was involved in 7 patients in the intervention group and 9 patients in the control group and the rest of the patients had their left shoulders involved; Chi-square test showed no significant difference in the involved shoulder between the two groups (P > 0.05). During the study, all the patients completed the primary medical therapy and the recommended exercises and no significant complications were noted. The mean and standard deviation of pain and disability scores, flexion, extension, and abduction, internal, and external rotation are shown in Table 1. Table 1 shows mean and standard deviation of pain and disability scores, flexion, extension, abduction, internal, and external rotation.
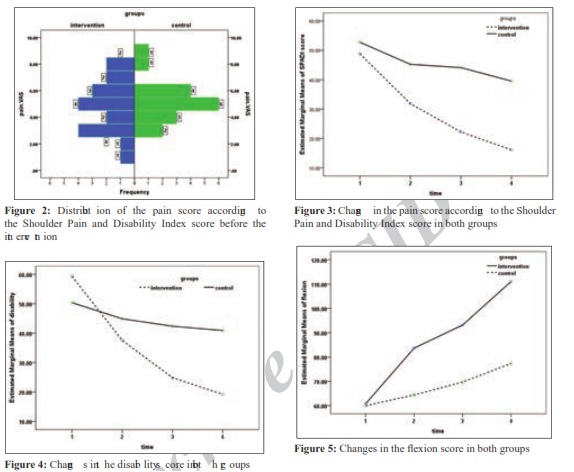
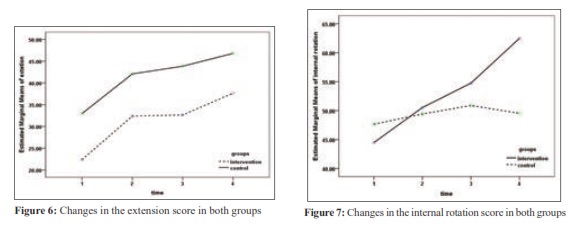
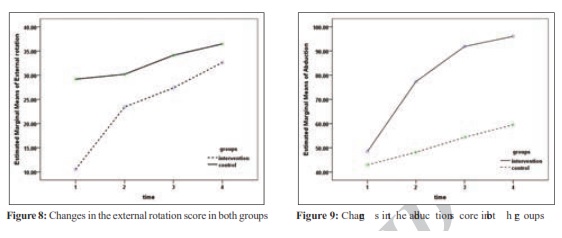
Independent t-test was performed on the data which revealed a difference in the mean pain and disability score of the SPADI questionnaire, flexion, extension, and abduction, internal, and external rotation of involved shoulder between two groups before and after the ESWT. Improvement was more satisfactory in the intervention group (P < 0.05). Although, the mean internal rotation in both groups was similar and no significant difference was observed in this variable between the two groups (P > 0.05). The fastest recovery in all mentioned values was obtained within 2 months after the intervention. After this period of time, the healing process slowed down. Minimal response to treatment was seen in patients with uncontrolled diabetes. Variable factors in the treatment period in both groups are shown in Figures 2-9.
problems, surgery methods have more complications. ESWT has positive results in orthopedic conditions
such as tendinitis, plantar fasciitis, lateral epicondilitis and rotator cuff disease. Since the
Rotator cuff problem is one of the predisposing factors for frozen shoulder and ESWT is effective in this condition, ESWT may also be useful in frozen shoulder. Durante et al. (2006) studied patients with similar conditions. One group of the patients were treated with extracorporeal shockwave combined with physiokinesiotherapy and the second group were treated with physiokinesiotherapy alone.[23] Patients received 2500 shocks from anterior and lateral directions with energy between 0.07 and 0.11 mJ/mm2 two sessions per week 2 weeks. All patients were followed for 6 months. About 30% of the patients showed excellent response, while 30% of patients showed poor response, as well. 10% of patients in the second group showed complete response. According to arthroscopic findings, adhesions occur more in the descendent fold and surrounding synovium, therefore, stimulation from anterior and posterior directions is more effective rather than the lateral direction. In the current study, the amount of the energy was higher than the study by Durante; other researches on the rotator cuff tendonitis have reported more effective responses with higher energy; therefore, it is better to increase the level of energy and decrease the number of shocks. In the present study, the better response to treatment was likely due to proper session intervals.
CONCLUSIONS
According to the findings of this study and in comparison with similar studies, ESWT has positive effects on acceleration of the healing process of frozen shoulder. Considering the significant side-effects of other therapies such as surgery, patients with frozen shoulder can take advantage of ESWT because of its noninvasive, safe nature, low costs, no need for hospitalization, fewer visits of patient in the hospital, and the lack of significant adverse events during the treatment.
RECOMMENDATION
Since systematic reviews on plantar fasciitis have revealed effective response to the use of the radial shockwave probe, the authors suggest that the efficacy of the radial probe in comparison with the probe focused on the treatment of frozen shoulder be evaluated in future studies.
ACKNOWLEDGMENT
This study was supported by a grant from Isfahan University of Medical Sciences (Grant no: 391061). The authors are grateful to the authorities of Kashani Hospital for their cooperation.
REFERENCES
- F ront ra G . A dhe s i ve c aps ul i ti s . E s s e nt i al s of P hys i c al M e di c i n e an d R e hab i l i tati on . 2 n d e P hi l ade l phi a: S aunde rs , E l s e vi e r; 2008. p. 49 - 54.
- B raddom R L . H an db ook of P hy s i c al M e di c i n e an d R e hab i l i tati on . 4 th e P hi l ade l phi a: W B S aun de rs ; 2 0 1 1 .
- 825.
- D al ton S E . T he s houl de r. I n: H oc hbe rg M , S i l m an A J , S m ol e n J S , e di tors . R he um atol og y . 3rd e d. T oron to: M os by; p. 615 - 30.
- D i as R , C utts S , M as s oud S . F roz e n s houl de B M J 2005; 331: 1453 - 6.
- Y an g J L , C han g C W , C he n S Y , W an g S F , L i n J J . M ob i l i z ati on te c hn i q ue s i n s ub j e c ts w i th f roz e n s houl de r s yndr om e : R andom i z e d m ul ti pl tre atm e nt tri al . J A m P hys T he r A s s oc P hys M e d 2013; 93: 1307- 15.
- B as f ord J R . T he rape uti c phys i c al age nt s . I n: D e l i s a J A , e di tor. P hys i c al M e di c i ne and R e habi l i tati P ri nc i pl e s an d P rac ti c e . P hi l ade l phi a: L i ppi n c ott W i l l i am s an d W i l ki ns ; 2005. p. 251 - 70.
- B e rghs B M , S ol e - M ol i ns X , B unke r T D . A rthros c opi c re l e as e of adhe s i vec aps ul i ti s . J S houl de r E l bow S urg 2004; 13: 180 - 5 .
L y n c hS A . S urg i c al an d n on s urg i c al tre atm e n t of adhe s i ve c aps ul i ti s . C urr O pi n O rthop 2002; 13: 271 - 4. tri al w i th ul tras on og raphi c an d s ub j e c ti v e outc om e as s e s s m e n ts . J R e s M e d S c i 2 0 1 2 ; 1 7 : 8 3 4 - 8 . R om pe J D , C ac c hi o A , W e i l L J r, F uri a J P , H ai s t J , R e i ne rs V, et al 3laQtar fascLa specLfic stretchLQJ versXs radi al shock - wave the rapy as i ni ti al tre atm e n t of pl ant ar f as c i opathy . J B one J oi nt S urg A m 2010; 92:2514- 22. R om pe J D , S c hoe l l n e r C , N af e B . E v al uati on of low eQerJy extracorporeal shock wave applLcatLoQ for tre atm e nt of c hroni c pl ant ar f as c i i ti s . J B one J oi nt S urg A m 2002; 84 - A : 335 - 41. 1 8 . S pe e d C A , N i c hol s D , R i c hards C , H um phre y s H , W i e s J T , B urn e t S , et al.





