 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Nikola
Nikola Kayser
Kayser Fusion
FusionSuprascapular Nerve Pulsed Radiofrequency for Chronic Shoulder Pain in a Pediatric Patient
- Type: Free
- Introduction
Shoulder pain is relatively common in the general pop- ulation and may result from an injury, inflammatory con- ditions, or a degenerative process. +e most common causes are related to rotator cuff disorders, glenohumeral and acromioclavicular capsulitis, or arthritis and joint instability [1, 2]. Most patients with chronic shoulder pain respond well to physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), and activity modification. Injection of a local anesthetic with steroids is also effective to alleviate in- flammation and to allow passive and active physical therapy [1, 3–5]. When the pain is intractable, a trial of pulsed radiofrequency (PRF) of the suprascapular nerve may be indicated as a means to delay or avoid surgery [6–8].
Pulsed radiofrequency was developed as a modification of continuous radiofrequency. In the latter, a high-frequency alternating current is applied to elevate the temperature
above 45–50°C to produce nonselective coagulative necrosis
of the nociceptive fibers. In PRF, on the other hand, high- voltage short bursts of current (20 ms) are followed by silent phases (480 ms) allowing diffusion of heat, maintaining the temperature in the target tissue below 42°C with the intention to produce prolonged “stunning” of nerve fibers without irreversible cell damage [8–11].
Pulsed radiofrequency (PRF) of the suprascapular nerve has shown efficacy in adults with chronic shoulder pain [7, 8, 10–13], but there are no reports of its use in children. We present a case were an ultrasound (US) guided PRF of the suprascapular nerve successfully alleviated refractory chronic shoulder pain in a pediatric patient.
2.Case Report
Informed consent was obtained from the patient and parents for the procedure and later for publication. A 53 kg, 14-year- old female, with a past medical history of septic arthritis of the left shoulder within the first month of life, presented with
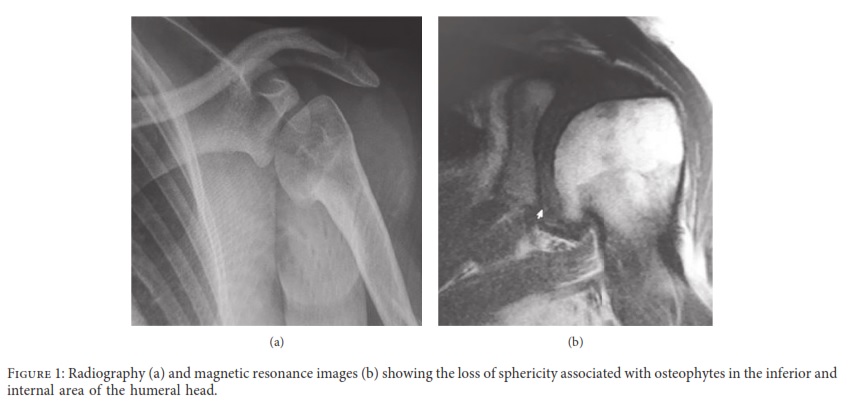
a complaint of progressive pain since age 12. Her pain had been refractory to analgesics including opioids, physical therapy, and intra-articular injection of local anesthetic and steroids for the past two years. +e patient was referred to the pain clinic after a trial of pregabalin and tramadol was unhelpful and 2 intra-articular injections of steroids and local anesthetics failed to provide analgesia. +e patient presented with severe pain (numeric rating scale ≥7/10), localized in the posterior and superior area of the gleno- humeral joint, exacerbated by passive and active abduction of the arm of more than 90 degrees. No swelling, peri- articular redness, or joint deformity were present. +e pain appeared to be somatic in nature, with no neuropathic features such as allodynia, paresthesia, burning sensation, or changes of the skin color. X-ray films and magnetic reso- nance images showed signs compatible with postinfectious arthritis including osteophytes in the inferior and internal area of the humeral head (Figure 1).
We performed diagnostic ultrasound-guided injection of the suprascapular nerve with bupivacaine 0.125% 6 ml and dexamethasone 4 mg resulting in complete pain relief for 15 days, returning to baseline severe pain scores afterwards. Given the favorable result of the diagnostic injection we decided to perform PRF of the suprascapular nerve.
+e procedure was performed in the operating room with the patient seated and monitored by an anesthesiolo-
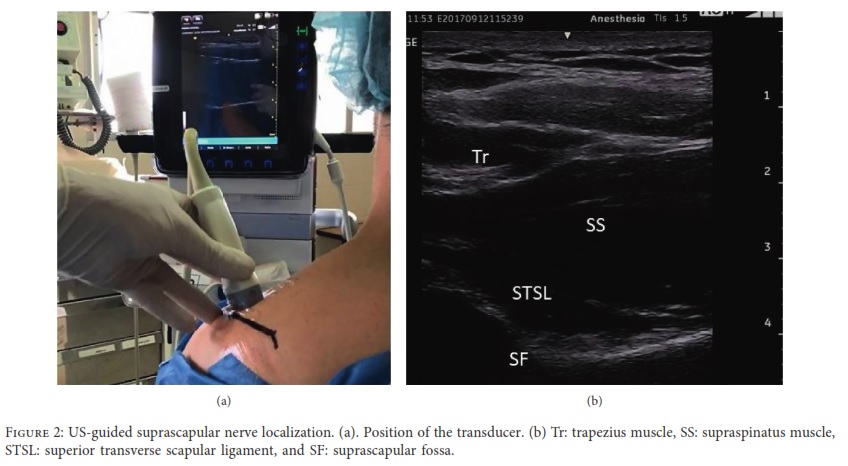
gist. Sedation was not required, and the patient tolerated the procedure well. A high-frequency linear transducer (10–15 Hz) was placed parallel and cephalad to the spine of the scapula (Figure 2(a)). +e probe was moved from cephalad to caudad until the trapezius and supraspinatus muscles were identified. +e suprascapular nerve was identified as a hyperechogenic structure in the suprascapular fossa deep to the superior transverse scapular ligament (Figure 2(b)). After skin infiltration with 3 ml of lidocaine
1%, a 10 cm radiofrequency needle, with a 10 mm active tip, was inserted in plane with the ultrasound beam and ad- vanced to reach the proximity to the nerve. A nerve stim- ulator was used as an additional nerve-finding modality. Sensitive stimulation (50–100 Hz at 0.4 Volts) elicited par- esthesia in the posterior aspect of the shoulder. Motor stimulation (2 Hz at 0.5 V) elicited muscle contraction of the supraspinatus and infraspinatus muscles. After adminis- tration of 2 ml of lidocaine 1%, PRF was applied to the suprascapular nerve at 45 V 42°C, in 2 cycles of 120 seconds.
+e procedure was well-tolerated. After 10 mins, the patient related complete resolution of the pain and was able to perform a full range of shoulder motions. She was dis- charged home with the instructions to use NSAIDs as needed. +e patient presented for follow-up appointments at 1, 3, and 6 months and reported only mild intermittent pain that responded to NSAIDs.
- Discussion
+is case report suggests that PRF may be considered for the management of chronic shoulder pain in children when conservative treatment and intra-articular injections of local anesthetic and steroids fail. In our case, a successful response was evidenced by an increased range of motion and im- provement of pain scores, consistent with the adult literature [7, 9–16]. After a single treatment, the pain was manageable with minimal analgesic requirements at the 6-month follow- up.
+e suprascapular nerve originates from the superior trunk of the brachial plexus. It provides 70% of the sensory innervation of the shoulder supplying the posterior and superior aspect of the glenohumeral joint, the joint capsule, and the acromioclavicular joint. It also provides motor innervation to the supra- and infraspinatus muscles [17].
+ere are concerns about using radiofrequency in children because of the potential risks of nerve injury that
may cause a permanent loss of function at an early age. However, several studies in adults have reported the safety of this technique making this treatment attractive. +e injury caused by PRF has a selective effect on small sensory fibers, A-δ and C-fibers [8–11]. It has been postulated that RF causes rectification of Na+ and K+ channels leading to a depolarization state which inhibits neural cells from reaching the action potential threshold in response to stimuli, therefore decreasing the neural transmission of painful sensations and ectopic discharges [18–21].
Ultrasound guidance offers the advantage of real-time imaging of the nerve and needle guidance, thus decreasing the potential for pneumothorax and vascular puncture, without the need of radiation exposure for the patients and personnel.
+e decision to perform this procedure despite limited previous experience in children was taken considering the
low risk potential and the possible benefits of avoiding surgery in view of the failed previous therapies. Procedural interventions in pediatrics are generally performed with scarce evidence and based on adult experience. +e positive results of this case report suggest that PRF may be effective in children and could be considered if the potential benefits outweigh the risks when noninvasive treatments fail.
Conflicts of Interest
+e authors declare that they have no conflicts of interest.
Acknowledgments
+e authors thank Dr. Navil Sethna, MD, for his assistance in reviewing the earlier draft and writing of the manuscript.
References
[1] S. Green, R. Buchbinder, R. Glazier, and A. Forbes, “Sys- tematic review of randomised controlled trials of interven- tions for painful shoulder: selection criteria, outcome assessment, and efficacy,” British Medical Journal, vol. 316, no. 7128, pp. 354–360, 1998.
[2] J. S. J. Picavet and J. S. A. G. Schouten, “Musculoskeletal pain in +e Netherlands: prevalences, consequences and risk groups, the DMC(3)-study,” Pain, vol. 102, no. 1-2, pp. 167–178, 2003.
[3] E. M. Shanahan, M. Ahern, M. Smith, M. Wetherall, Bresnihan, and O. FitzGerald, “Suprascapular nerve block (using bupivacaine and methylprednisolone acetate) in chronic shoulder pain,” Annals of the Rheumatic Diseases, vol. 62, no. 5, pp. 400–406, 2003.
[4] T. H. Dahan, L. Fortin, M. Pelletier, M. Petit, Vadeboncoeur, and S. Suissa, “Double blind randomized clinical trial examining the efficacy of bupivacaine supra- scapular nerve blocks in frozen shoulder,” $e Journal of Rheumatology, vol. 27, no. 6, pp. 1464–1469, 2000.
[5] P. C. Vecchio, A. O. Adebajo, and B. L. Hazleman, “Supra-scapular nerve block for persistent rotator cuff lesions,” $e Journal of Rheumatology, vol. 20, no. 3, pp. 453–455, 1993. [6] J. J. Lee, J. S. Yang, S. M. Hwang, S. H. Kang, J. S. Jang, and J. Choi, “Effect of pulsed radiofrequency neuromodulation on clinical improvements in the patients of chronic intractable shoulder pain,” Journal of Korean Neurosurgical Society, vol. 54, no. 6, p. 507, 2014.
[7] Y.-T. Wu, C.-W. Ho, Y.-L. Chen, T.-Y. Li, K.-C. Lee, and L.-C. Chen, “Ultrasound-guided pulsed radiofrequency stimulation of the suprascapular nerve for adhesive capsu- litis,” Anesthesia & Analgesia, vol. 119, no. 3, pp. 686–692, 2014.
[8] A. Liu, W. Zhang, M. Sun, C. Ma, and S. Yan, “Evidence-based status of pulsed radiofrequency treatment for patients with shoulder pain: a systematic review of randomized controlled trials,” Pain Practice, vol. 16, no. 4, pp. 518–525, 2016.
[9] T. Vanneste, A. Van Lantschoot, K. Van Boxem, and J. Van Zundert, “Pulsed radiofrequency in chronic pain,” Current Opinion in Anaesthesiology, vol. 30, no. 5, pp. 577– 582, 2017. [10] P.-C. Liliang, K. Lu, C.-L. Liang, Y.-D. Tsai, C.-H. Hsieh, and H.-J. Chen, “Pulsed radiofrequency lesioning of the supra-
scapular nerve for chronic shoulder pain: a preliminary report,” Pain Medicine, vol. 10, no. 1, pp. 70–75, 2009.
[11] N. Luleci, U. Ozdemir, K. Dere, H. Toman, E. Luleci, and Irban, “Evaluation of patients’ response to pulsed radio frequency treatment applied to the suprascapular nerve inpatients with chronic shoulder pain,” Journal of Back andMusculoskeletal Rehabilitation, vol. 24, no. 3, pp. 189–194,2011.
[12] K. Keskinbora, I. Aydinli, J. S. Jang et al., “Pulsed radiofrequency applied to the suprascapular nerve in painful cufftear arthropathy,” Journal of Shoulder and Elbow Surgery, vol. 17, no. 3, pp. 189–194, 2009.
[13] T. P. C. Kane, P. Rogers, J. Hazelgrove, S. Wimsey, andD. Harper, “Pulsed radiofrequency applied to the supra scapular nerve in painful cuff tear arthropathy,” Journal of Shoulder and Elbow Surgery, vol. 17, no. 3, pp. 436–440, 2008.
[14] E. Sir and S. Eksert, “Ultrasound-guided pulsed radio frequency neuromodulation of the suprascapular nerve in partial rotator cuff tears,” Turkish Journal of Medical Sciences,vol. 49, no. 5, pp. 1524–1528, 2019.
[15] T. Ergo¨nenç and S. G. Beyaz, “Effects of ultrasound-guidedsuprascapular nerve pulsed radiofrequency on chronicshoulder pain,” MedicalUltrasonography, vol. 20, no. 4,461–466, 2018.
[16] J. Yan and X. M. Zhang, “A randomized controlled trial of ultrasound-guided pulsed radiofrequency for patients with frozen shoulder,” Medicine (Baltimore), vol. 98, no. 1, Article ID e13917, 2019.
[17] O. C. Aszmann, A. L. Dellon, B. T. Birely, and G. McFarland, “Innervation of the human shoulder joint and its implications for surgery,” Clinical Orthopaedics and Related Research, vol. 330, pp. 202–207, 1996.
[18] E. R. Cosman and E. R. Cosman, “Electric and thermal field effects in tissue around radiofrequency electrodes,” Pain Medicine, vol. 6, no. 6, pp. 405–424, 2005.
[19] A. Cahana, J. Van Zundert, L. Macrea, M. van Kleef, and Sluijter, “Pulsed radiofrequency: current clinical and bi ological literature available,” Pain Medicine, vol. 7, no. 5,411–423, 2006.
[20] R. Munglani, “+e longer term effect of pulsed radiofrequency for neuropathic pain,” Pain, vol. 80, no. 1-2, pp. 437–439,1999.
[21] D. Abejo´n and E. Reig, “Is pulsed radiofrequency a Neuro modulation technique?” Neuromodulation: Technology at the Neural Interface, vol. 6, no. 1, pp. 1–3, 2003.





