 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Nikola
Nikola Kayser
Kayser Fusion
FusionUltrasound-guided pulsed radiofrequency for chronic shoulder pain: a prospective study
- Type: Free
Abstract
Background and objectives: Chronic shoulder pain is a frequent cause of suffering and impaired quality of life. Treatment includes non-pharmacological and pharmacological therapies, and interventional procedures such as suprascapular nerve blocks and radiofrequency. This prospec- tive study aims to evaluate the efficacy of ultrasound-guided pulsed radiofrequency of suprascapular nerve for chronic shoulder pain in a clinical setting.
Methods: Therapeutic efficacy was evaluated through pain intensity using numeric pain rating scale at baseline, immediately, 3, and 6 months after, and patient’s motor function improve- ment. The secondary outcome was patient satisfaction.
Results: A total of 34 patients were enrolled and all patients presented a reduction in the numeric pain rating scale immediately after treatment. Pain reduction from baseline to 6 months after the procedure was 34.4% and 36.9% static and dynamic, respectively. The median percentage reduction was statistically significant immediately, 3 and 6 months after. There was also an improvement in range of motion, 39.6% in abduction, 24.1% in flexion, and 29.5% in extension. Ninety percent of patients reported patient’s global impression of change superior to six.
Conclusion: This study concludes that ultrasound-guided pulsed radiofrequency of suprascapu- lar nerve reduces pain intensity for at least 6 months, accompanied by improvement of motor function and higher levels of patients’ satisfaction. Therefore, this technique represents a valid analgesic approach to chronic shoulder pain.
© 2021 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by- nc-nd/4.0/).
Introduction
Shoulder disorders are the third most prevalent type of musculoskeletal complaint in adults. They can significan- tly impact life quality, entailing considerable health costs, disability, and work absenteeism. Chronic shoulder pain prevalence ranges from 15.5% to 41% in the general pop- ulation, increasing with age, and is higher for women.1,2,4,5 Shoulder pain etiology can be attributable to intrin- sic disorders, comprising the rotator cuff, glenohumeral, acromioclavicular, biceps tendonitis, infection, shoulder instability, or as extrinsic shoulder pain such as referred
pain, polymyalgia rheumatic, and malignancy.2,3,5,6
The nerves supplying the shoulder joint arise from the brachial plexus. The suprascapular nerve supplies 70% of the sensory innervation of the shoulder joint, whereas the remaining 30% is supplied by the subscapular nerve, axillary nerve, and lateral pectoral nerve.5 The suprascapular nerve is a mixed nerve, both motor and sensitive, originated in the upper trunk of brachial plexus, C5 and C6 roots. It runs infe- rior, posterior, and laterally to reach the supraspinous fossa in the scapula. The sensitive components innervate the pos- terior and superior shoulder capsule, glenohumeral, and the acromioclavicular joint. The motor components innervate the supra and infraspinatus muscles.
Shoulder pain treatment involves a multimodal approach, including non-pharmacological (physical therapy, tran- scutaneous electric nerve stimulation), pharmacological therapies, and interventional procedures such as intra- articular steroid injections, suprascapular nerve blocks, radiofrequency of suprascapular nerve and surgery.7,9
Pulsed radiofrequency was first reported in 1998 as a non-neurolytic lesioning method delivering an electri-
cal field and heat bursts (temperature < 42 ◦C) for pain relief without evidence of neural damage.8,10 Previous
studies demonstrate significant pain relief and functional improvement in patients with chronic shoulder pain of a wide range of etiologies.11,12 Throughout most studies, authors use fluoroscopy or computed tomography-guided techniques. However, ultrasound-guidance radiofrequency has advantages over other imaging modalities, for instance, portability, real-time assessment and dynamic evaluation, limited trauma, and avoidance of patient and physician radiation exposure.13---15 Only a few previous studies have evaluated ultrasound efficacy of suprascapular nerve pulsed radiofrequency and patient satisfaction.15---18
In this regard, our main objective was to prospectively evaluate the efficacy of ultrasound-guided suprascapular nerve pulsed radiofrequency for chronic shoulder pain treat- ment in a chronic pain unit. The primary outcome was efficacy using pain intensity and motor function improve- ment. The secondary outcome was patient satisfaction.
Methods
This prospective study was conducted at our chronic pain unit between May 2016 and December 2019. A total of thirty- six patients were submitted to a diagnostic block, from which thirty-four patients were included in this study as they matched the inclusion criteria.
Ethics statement
The data was collected after receiving approval from the Ethical Committee of our institution. All patients submit- ted to the suprascapular block and pulsed radiofrequency received oral and written information and signed informed consent before the procedure.
Inclusion criteria
The following inclusion criteria were used: diagnosis of chronic shoulder pain (> 6 months); over 18 years of age; non-pregnancy; non-allergy to local anesthetic or corticos- teroids; non-local or systemic infection; reduction of at least 50% in pain intensity after previous ultrasound-guided suprascapular nerve block.
Patient, clinical and outcome variables
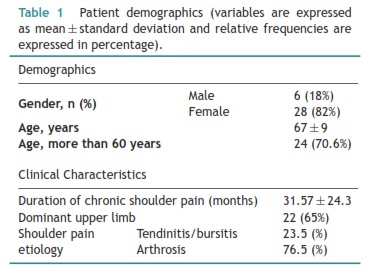
Patient demographics
The following information was collected from patients: gender, age, chronic pain duration, dominant upper limb, and shoulder pain etiology.
Numeric pain rate scale
Pain intensity was assessed at baseline, immediately, three and six months after using the Numeric Pain Rate Scale (NPRS). This unidimensional pain instrument consists of a horizontal line with a beginning point marked as zero (‘‘no pain’’) and at the opposite end, marked as 10 (‘‘worst pain possible’’). Patients report the number which best repre- sents the pain they are/were feeling. Generally, pain in the 1---3 category is ranked as mild pain, 4---6 as moderate pain and 7---10 as severe pain.
Motor function evaluation
Static and dynamic patient motor function was assessed by the same rehabilitation nurse specialist, before and after suprascapular radiofrequency, measuring range of motion (abduction, flexion, and extension) using a goniometer. Mus- cle strength was also assessed.
SPADI
A validated Portuguese score of Shoulder Pain and Disability Index (SPADI-VP) was used at baseline as a secondary clin- ical outcome.19 It contains thirteen issues related to pain and disability associated with shoulder disorders. For each question, there is a scale of 0 to 10. Zero indicates activ- ity without difficulty and ten corresponds to the condition where the individual is not capable of carrying out the pro- posed activity. The maximum score of the questionnaire is 80 points. The individual obtained score is converted into a percentage, with 100% being the worst condition of shoulder dysfunction. SPADI was designed to measure the impact of shoulder pathology in terms of pain and disability and assess how these metrics evolve.20
Patient satisfaction
Patient satisfaction is a good indicator of the quality of health care. This was evaluated using the Patient’s Global

Impression of Change Validated Portuguese (PGIC-VP) ques- tionnaire immediately and six months after the procedure. In this unidimensional tool, patients report their treatment improvement on a 7-item scale, with 1 representing ‘‘no change’’ and 7 representing ‘‘a great deal better’’.21
Ultrasound-guided pulsed radiofrequency
All procedures were performed by the same anesthesiologist with expertise in chronic pain management and ultrasound- guided interventions, using Acuson ultrasound from Siemens P300®, linear probe 12 MHz. Patients were placed in a sit- ting position and standard monitoring was applied. Under aseptic conditions, the linear transducer was positioned just cephalad and parallel to the scapular spine. The suprascapu- lar nerve was identified as a hyperechoic structure below the transverse scapular ligament in the scapular notch. A 22 G 60-mm radiofrequency needle was then advanced under ultrasound guidance toward the scapular notch by using the in-plane approach (Fig. 1). Sensory stimulation was performed with 10---200 Hz, 1 ms pulse width, up to
- volts and the patients reported paraesthesia in the shoul- der After motor stimulation (2 Hz, 1 ms pulse width, up to 1 volt), contractions of the infra- and supraspinatus muscles were observed. Pulsed radiofrequency lesioning was then performed for 180 seconds (2 Hz, 30 ms pulse width, temperature < 42 ◦C). Thirty minutes after the procedure, pain intensity was evaluated using NPRS and patients were discharged home. A chronic pain appointment was schedule one, three, and six months after the procedure.
Statistical analysis
From the Shapiro-Wilk test, it was assessed that the data does not follow a normal distribution. Thus, the correlation
coefficients were calculated using the Spearman test to quantify the association between static and dynamic base- line NPRS and immediate, three and six months NPRS, and among NPRS and dominant arm and between NPRS and PGIC- VP. The accepted level of significance for the correlation was p < 0.01 for a strong correlation and p < 0.05 for moderate correlation.
Treatment efficacy was quantified by calculating absolute differences and percentage change from baseline. For each patient, a response was considered clinically relevant if the NPRS was reduced by at least 30% relative to baseline, as is standardly accepted.22
Results
Of thirty-six patients, two were excluded from the study because it was not observed a reduction of at least 50% in pain intensity after ultrasound-guided suprascapular nerve block (did not meet the first inclusion criterion). The demographic characteristics of the thirty-four patients are presented in Table 1.
Changes in NPRS
We started by analyzing the change in static and dynamic NPRS between baseline and immediately after the proce- dure (Table 2). All patients presented a reduction in NPRS immediately after treatment. Of the patients, 94.1% and 91.2% presented a clinically significant reduction in static and dynamic NPRS, respectively. Complete pain relief (NPRS lower or equal to 1) was obtained in 76.5% and 23.5% of patients, regarding static and dynamic NPRS, respectively. Median percentage reduction in the NPRS immediately after the procedure of 86.8 and 69.6% static and dynamic, respec- tively.
To characterize treatment efficacy in the long-term, per- centage reduction from baseline to 3 months after the procedure was 54.9% and 53.7%, static and dynamic, respec- tively (Fig. 2). Then it was mandatory to see if a persistent notorious reduction could be observed over time. To this end, we evaluated NPRS reduction after six months (34.4% and 37.0%, static and dynamic). The median percentage reduction was also statistically significant (p < 0.01 one-
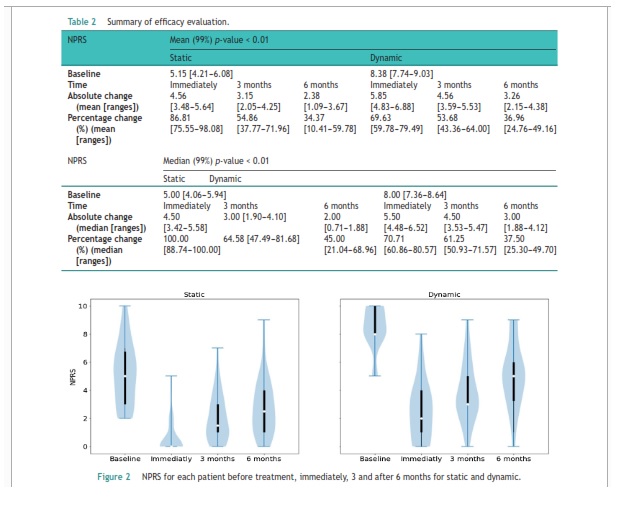
sided Wilcoxon signed-rank test); this gauge the treatment effectiveness.
A strong correlation with high statistical significance was found between the reduction of static NPRS immediately, 3 and 6 months, and baseline. A strong correlation with high statistical significance was also found among static and dynamic reduction of NPRS after 6 months. Low correlation and high statistical significance were found among PGIC-VP and higher reduction in NPRS for both static and dynamic. A correlation between the dominant arm and the other variables was not found.
SPADI-VP
SPADI was developed to measure current shoulder pain and disability. In our study median SPADI score was 35.17, with a minimum of 27 and a maximum of 65.7.
Motor function
Treatment efficacy was also analyzed regarding improvement of motor function. Therefore, changes in the range of motion (flexion, abduction, and extension) at baseline and after six months were compared. The median baseline of flexion abduction and extension were 12.5o, 22.5o and 20o, respectively. Increased 39.6% in flexion, 24.1% in abduction, and 29.5% in extension after six months.
Patient satisfaction
Regarding self-report measure PGIC-VP: 50% scored ‘‘7’’ representing ‘‘a great deal better’’; 40% scored ‘‘6’’ indicating ‘‘better’’; 10% scored ‘‘5’’ representing moderately better. Thus, 90% of our patients had a clinically significant improvement.
Discussion
These results indicate that ultrasound-guided pulsed radiofrequency of suprascapular nerve for chronic shoulder pain provide a statistically significant reduction in static and dynamic pain score and range of motion (flexion, abduc- tion, and extension), and the effect persisted for at least 6 months.
Our study describes an aging population, with 70.6% aged over 60 years. Older individuals have a higher incidence of chronic shoulder pain, mainly due to degenerative rotator cuff pathologies. Recently, a change of the morphology of the suprascapular nerve has been identified in patients with supraspinatus tendon full-thickness tear, resulting in nerve entrapment,23 rephrasing the importance of suprascapular nerve interventions as a fundamental tool in chronic shoulder pain treatment. However, as the effect of suprascapular nerve block has a limited duration, diagnostic blocks should be performed to identify patients who should proceed to the treatment. A patient with greater than 50% pain relief is considered to have a positive diagnostic block.14,15 While intra-articular injections have diagnostic value, they have less prognostic value for radiofrequency success.24,25
The mechanism pointed for pulsed radiofrequency long- term pain relief is the neuromodulatory effect created via alternating the expression of a gene such as c-fos in pain pro- cessing neurons.26 Pulsed radiofrequency of suprascapular nerve was applied by Rohof in 2002 with a blind technique.27 Peripheral pulsed radiofrequency has gained acceptance by pain control with the non-destructive mechanism. Both ther- mal and pulsed radiofrequency ablation of the suprascapular nerve have been described to treat chronic shoulder pain, but there is a theoretical concern of post-ablation weak- ness in the supraspinatus and in infraspinatus muscles.28 Research reported that pulsed radiofrequency of supras- capular nerve was effective in treating chronic shoulder pain. Despite the extensive use of fluoroscopy or computed- tomography guidance in literature,29---31 recent studies start adopting ultrasound guidance.15,17 Also, some studies did not characterize long-term treatment efficacy.9
The etiology of chronic shoulder pain is diverse, as is its treatment. Rotator cuff pathology treatment has been studied with mixed outcomes and little research has been done to evaluate its efficacy in other shoulder etiologies.15,17 In our work, there was no significant difference in long- term efficacy in both group etiologies (tendinitis/bursitis and arthrosis) for chronic shoulder pain, as such, we can- not pinpoint a specific metric that most prominently factors for the existence of either arthrosis or tendinitis.
Patient satisfaction with chronic shoulder pain treatment has received less attention in previous studies. Satisfaction with treatment of chronic pain is not merely a matter of pain relief. It is important to distinguish satisfaction with care of satisfaction with improvement after treatment. Patient sat- isfaction is a subjective experience; it can be defined as the emotional feeling resulting from the comparison between the actual perceived performance and quality of the treat- ment with the original expectations. It is frequently used as an indicator of meaningful change in treatments for chronic pain. The definition of clinically significant change suggests that PGIC-VP values of 6 or more correlate best with actual
change. According to PGIC-VP, 90% of our patients had a clin- ically significant improvement. In our study, patients with higher reduction in NPRS were most closely correlated with PGIC-VP status, regardless of initial pain intensity.
Our study caveat is 2-fold: it was conducted using a small sample size and it lacks a control group. A longer-term follow-up would be desirable.
Future research is needed to assess the best treatment approach for various chronic shoulder pain etiologies.
Conclusions
Ultrasound-guided suprascapular nerve radiofrequency is a safe and effective technique for treating chronic shoulder pain, providing significant improvement in NPRS during at least 6 months, accompanied with improvement of motor function and higher levels of patient satisfaction. Therefore, this technique represents a valid analgesic approach to a multimodal treatment strategy of chronic shoulder pain.
Future randomized control trials are warranted for vali- dating these results.
Conflicts of interest
The authors declare no conflicts of interest.
References
- Picavet H, Schouten Musculoskeletal Pain in the Netherlands: Prevalences, Consequences and Risk Groups, the DMC(3)-study. Pain. 2003;102:167---78.
- Greving K, Dorrestijn O, Winters J, et al. Incidence, preva- lence, and consultation rates of shoulder complaints in general practice. Scand J Rheumatol. 2012;41:150---5.
- Pribicevic M. The epidemiology of shoulder pain: a narrative review of the literature. IntechOpen. 2012:147---86.
- Fernandes MR, Barbosa MA, Sousa ALL, Ramos GC. Suprascapular nerve block: important procedure in clinical practice. Braz J Anesthesiol. 2012;62:96---104.
- Mitchell C, Adebajo A, Hay E, Carr Shoulder pain: diagnosis and management in primary care. BMJ. 2005;331:1124---7.
- Liliang PC, Lu K, Liang CL, Tsai YD, Hsieh CH, Chen Pulsed radiofrequency lesioning of the suprascapular nerve for chronic shoulder pain: a preliminary report. Pain Med. 2009;10:70---5.
- Eyigor C, Eyigor S, Korkmaz OK, Uyar M. Intra-articular cor- ticosteroid injections versus pulsed radiofrequency in painful shoulder: a prospective, randomized, single-blinded study. Clin J Pain. 2010;26:386---92.
- Cosman ER. A comment on the history of the pulsed radiofre- quency technique for pain therapy. J Am Soc Anesthesiol. 2005;103:1312.
- Chang PH, Chen YJ, Chang KV, Wu WT, Öz¸cakar Ultrasound measurements of superficial and deep masticatory muscles in various postures: reliability and influencers. Scientific Reports. 2020;10:2045---322.
- Hsu PC, Chang KV, Wu WT, Wang JC, Öz¸cakar L. Effects of ultrasound-guided peritendinous and intrabursal corticosteroid injections on shoulder tendon elasticity: a post hoc analysis of a randomized controlled Arch Physical Med Rehabilitation. 2021;102:905---13.
- Wu YT, Ho CW, Chen YL, Li TY, Lee KC, Chen LC. Ultrasound- guided pulsed radiofrequency stimulation of the suprascapular nerve for adhesive Anesth Analg. 2014;119:686---92.
- Sir E, Eksert S. Ultrasound-guided pulsed radiofrequency neu- romodulation of the suprascapular nerve in partial rotator cuff tears. Turk J Med Sci. 2019;49:1524---8.
- Ergonenc T, Beyaz Effects of ultrasound-guided suprascapu- lar nerve pulsed radiofrequency on chronic shoulder pain. Med Ultrason. 2018;20:461---6.
- Huang CC, Tsao SL, Cheng CY, Hsin MT, Chen Treating frozen shoulder with ultrasound-guided pulsed mode radiofrequency lesioning of the suprascapular nerve: two cases. Pain Med. 2010;11:1837---40.
- Guerreiro JA, Proen¸ca I, Moura N, Cartuxo A. Adapta¸cão transcultural do shoulder rating questionnaire para a língua por- tuguesa (srq-pt): tradu¸cão; valida¸cão; análise da consistência interna e replicabilidade. Ifisionline. 2011;1:5---18.
- Bautz-Holter E, Juel NG, Ekeberg OM, Tveitå EK. Responsive- ness of the Shoulder Pain and Disability Index in Patients with Adhesive Capsulitis. BMC Musculoskeletal Disorders. 2008;9.
- Boonstra AM, Preuper HRS, Balk GA, Stewart Cut-off points for mild, moderate, and severe pain on the visual analogue scale for pain in patients with chronic musculoskeletal pain. Pain. 2014;155:2545---50.
- Chang KV, Hung CY, Wu WT, Han DS, Yang RS, Lin CP. Com- parison of the effectiveness of suprascapular nerve block with physical therapy, placebo, and intra-articular injection in management of chronic shoulder pain: a meta-analysis of randomized controlled Arch Physical Med Rehabilitation. 2016;97:1366---80.
- Wu WT, Chen LR, Chang HC, Chang KV, Öz¸cakar L. Quantita- tive ultrasonographic analysis of changes of the suprascapular nerve in the aging population with shoulder Front Bioeng Biotechnol. 2021;9:121.
- Cohen SP, Moon JY, Brummett CM, White RL, Larkin Medial branch blocks or intra-articular injections as a prognostic tool before lumbar facet radiofrequency denervation: a multicenter, case-control study. Reg Anesth Pain Med. 2015;40:376---83.
- Eckmann MS, Johal J, Bickelhaupt B, et al. Terminal sensory articular nerve radiofrequency ablation for the treatment of
chronic intractable shoulder pain: a novel technique and case series. Pain Med. 2020;21:868---71.
- Liu A, Zhang W, Sun M, Ma C, Yan Evidence-based status of pulsed radiofrequency treatment for patients with shoulder pain: a systematic review of randomized controlled trials. Pain Pract. 2016;16:518---25.
- Rohof Radiofrequency treatment of peripheral nerves. Pain Pract. 2002;2:257---60.
- Simopoulos TT, Nagda J, Aner MM. Percutaneous radiofrequency lesioning of the suprascapular nerve for the management of chronic shoulder pain: a case J Pain Res. 2012;5:91---7.
- Gofeld M, Restrepo-Garces CE, Theodore BR, Faclier Pulsed radiofrequency of suprascapular nerve for chronic shoulder pain: a randomized double-blind active placebo-controlled study. Pain Pract. 2013;13:96---103.
- Korkmaz OK, Capaci K, Eyigor C, Eyigor S. Pulsed radiofrequency versus conventional transcutaneous electrical nerve stimula- tion in painful shoulder: a prospective, randomized Clin Rehabil. 2010;24:1000---8.
- Taverner M, Loughnan Transcutaneous pulsed radiofrequency treatment for patients with shoulder pain booked for surgery: a double-blind, randomized controlled trial. Pain Practice. 2014;14:101---8.
- Domingues L, Cruz Eb. Adapta¸cão Cultural e Contributo para a Valida¸cão da Escala Patient Global Impression of Ifi- sionline. 2011;2:31---7.
- Wyrwich KW, Wolinsky FD. Identifying meaningful intra- individual change standards for health-related quality of life measures. J Evaluation Clin Practice. 2000;6:39---49.
- Hirsh At, Atchison Jw, Berger Jj, et al. Patient satisfaction with treatment for chronic pain:predictors and relationship to compliance. Clin J Pain. 2005;21:302---10.
- Cohen SP, Baber ZB, Buvanendran A, et al. Pain manage- ment best practices from multispecialty organizationsduring the COVID-19 pandemic and public health crises. Pain Med. 2020;21:1331---46.





