Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Tesla
Tesla Nikola
Nikola Kayser
Kayser Fusion
FusionTecar therapy in the treatment of acute and chronic pathologies in sports
- Type: Free
- Download
Tecar therapy in the treatment of acute and chronic pathologies in sports
Abstract
This study utilized Tecar® therapy, a capacitive and/or resistive energy transfer system that operates within the long wave radio frequency range in the treatment of acute and chronic musculo-articular pathology in athletes. Tecar® therapy is characterized by the transfer of energy within tissues by using a capacitive electrode covered by an insulator and a resistive electrode conductor, following the mechanism of a condenser. The device used is composed of a generator that distributes signals at a frequency of 0.5 MHz at a maximum power of 300 watts.
The study observed 327 subjects (120 females, 207 males) between 18 and 60 years of age with acute and chronic sports pathologies. They were divided into two groups, one comprised of 68 cases of acute pathologies which had not been previously treated, and another comprised of 259 cases of chronic pathologies treated by various methods. The sessions were started with resistive treatment with an electrode positioned on the area to be treated for 10 minutes (5 minutes for muscular pathology), followed by another 10 minutes (15 minutes for muscular pathology) with a capacitive electrode applied.
The progression of symptoms was clinically monitored and evaluated by an independent observer using the Steinbroker index modified for athletic activity and with the visual analogue scale (VAS) from 0 to 10 where 0 corresponds to no pain and 10 corresponds to intolerable pain. The pathologies treated were articular, muscular, and tendinous, and among these, those that displayed a more marked change in functional class were the muscular pathologies.
The results obtained indicate that Tecar® therapy is a useful tool in the treatment of sports pathologies of the bone, joints, and muscles. It compares with other therapies in terms of the presence or absence of certain positive effects but it also has distinct characteristics that are effective even where other treatments have failed.
KEYWORDS: Hyperthermia, musculo-articular pathology, vasodilatation
Although a relatively broad range of physiotherapeutic equipment is currently in use, including various devices for generating electric currents induced or transmitted directly to the human body, there are various articular, tendinous, and myoenthesic pathological processes that are particularly resistant to treatment and significantly limit the possibility of athletic activity both at competitive and amateur level.
The possibility that a new method of energy transfer at a deep level could also be useful in certain cases to shorten and resolve pathologies limiting athletic performance as well as daily activity seems to be, at the very least, worthy of consideration.
Hyperthermia was developed to treat, in conjunction with other chemical and physical means, tumorous masses in order to destroy the most central cells, which are less metabolically active and have little contact with circulating blood. One of the methods used is hyperthermia induced by radio frequency1. In addition to central necrosis, some observations indicated a reduction in peripheral oedema around the carcinomatous mass2 and have suggested that this method could also be used in tissues subject to inflammatory reactions with the required proportions of intensity and time. In this case, the blood flow, accentuated by increase in temperature, could, with an increase in caloric exchange, avoid reaching temperatures that could cause cellular necrosis, observed in the therapy of tumours.
In 1953, Lehmann3 had already demonstrated how temperatures from 40 to 45ºC could have therapeutic effects in various pathological conditions, but temperatures of 44-45ºC should be maintained for only brief periods of time.
Recently, a system for capacitive and resistive energy transfer known as Tecar® therapy has been developed, operating within the long wave radio frequency range at 0.5 MHz, hence lower than the frequencies used in short wave diathermy (27.1 MHz), and higher than the frequencies that can cause muscle contractions. Tecar® therapy has its own distinguishing characteristic in the field of diathermy equipment, by stimulating energy transfer within tissues by using a capacitive or resistive electrode.
The first electrode (Capacitive) is covered by an insulator, and the second (Resistive) is a conducting electrode. In the first case, let us imagine a condenser with two frameworks, where one is a metal conductor plate (the dielectric is opposite its surface), and the other is a type-2 conductor, formed from the biological tissue and from another metal conductor plate (Return Plate) that closes the circuit.
A type-2 conductor is characterized by displacement currents rather than conduction, and the charged particles tend to have a higher density in the vicinity of the dielectric and their energy tends to increase progressively from the counter electrode to the insulated electrode with resulting increase in temperature. Hence, there is a greater increase in energy in muscles positioned closely to the insulated electrode.
If the insulated electrode is held still, the sensation of heat on the skin on contact quickly becomes intolerable, thus the treatment involves the slow and continuous movement of the electrode in a circular fashion and subsequent displacements equal to the electrode beam.
In the case of a resistive electrode, the circuit is formed in which the framework is comprised of an electrode which is a type-1 conductor and underlying biological tissues with characteristics of type-2 conductors, a dielectric formed from bone tissue, a second framework formed from the biological tissue conductor and a (Return Plate) that closes the circuit.
In this case, the higher energy density is close to the bone surfaces, hence at the level of insertion of the tendons, ligaments, and joints. In fact, in this case, the active electrode can be kept still and the sensation of increase of energy will be felt, above all, in cases of insertion-point or articular pathology at this level. All of the conducting structures subjected to electromagnetic waves will have an increase in energy as an increase in ionic movement and where the waves accumulate, in each case there will be an increase in temperature.
The increasing power of the generator is perceived by the patient as excessive, and this is also the case with a resistive electrode. In fact, it can be observed that the skin temperature with the use of a resistive electrode progressively diminishes towards the counter electrode. For example, in the treatment of the Achilles tendon, the maximum skin temperature is shown at the heel (table 1).
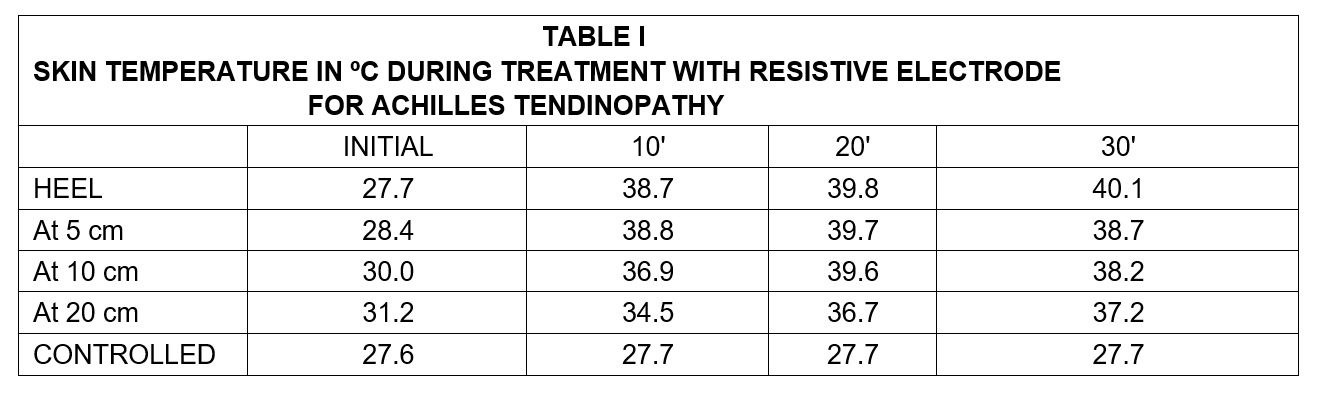
The temperature rises rapidly in the first 10 minutes and more slowly in the subsequent minutes. After 20 minutes, the increments are very slight and in some areas the temperature tends to rise depending on the circulatory flow.
The appropriate positioning of electrode (smaller with higher current density) and counter electrode allows for the treatment of various areas of the body. In particular, for treatment of muscles, a capacitive electrode is positioned with counter electrode (Return Plate) that closes the circuit on the opposite side of the limb, while for treatment of joints, the electrode is positioned on one side of the joint and a counter electrode on the opposite side.
The physiological effects of this increase in energy are represented by:
- Increase in extensibility of the collagenous tissue due to reduction in viscosity.
- Reduction of pain due to ant-irritant action or release of endorphins.
- Reduction of muscular spasms and contractions due to reduced activity of secondary efferents.
- More rapid and complete dissociation of oxygen from haemoglobin with more availability, accompanied by a reduction in activation energy of important chemical and metabolic reactions.
- Vasodilatation with increase of local blood flow contributing to the re-supply of oxygen and nutritional substances as well as the removal of catabolytes.
- Quickening of re-absorption of haemorrhagic masses.
Other possible effects related to the specific action of the electromagnetic field may be envisaged but have not been demonstrated
Materials And Methods
The apparatus used is comprised of a generator that supplies a signal at the frequency of 0.5 MHz and a maximum power of 300 watts (HCR900).The power can be regulated by controlling the quantity of transferred energy and the relative biological action. The active electrodes are formed of metallic elements of various dimensions (from a few centimetres to a few millimetres), some of which are completely covered by a special ceramic material that functions as a dielectric.
The counter electrode (Return Plate) that closes the circuit consists of a metal plate that is applied in opposition or a cylinder that is clasped. The area to be treated is covered by a light layer of a special gel that has the sole function of smoothing physical contact between the electrode and the skin.
The session begins with resistive treatment with an electrode that is positioned on the area to be treated, kept fixed for 10 minutes (5 minutes in cases of muscular pathology) with power regulated in order to obtain the maximum skin temperature acceptable to the patient without creating any pain (repeated adjustments may be necessary to achieve this).
This is followed by application with capacitive electrode for 10 minutes (15 minutes in cases of muscular pathologies). In this case, the electrode must be continually moved by the operator in circular motions to avoid disturbing skin sensations from the excessive local heat.
A total of 10 sessions per day were carried out on successive days with a pause of two days at the end of the week.
The 327 subjects (120 females and 207 males) were between 18 and 60 years of age and had acute and chronic pathologies from sports activity.
They were subdivided into two groups; one comprised of 68 subjects with acute pathologies that were not previously treated and the other comprised of 259 subjects with chronic pathologies that were already treated a number of times with various treatments (FANS, steroid injections, US, ionophoresis, etc.).
No other physical or pharmacological treatment was used during the phase of Tecar® therapy. In cases of acute pathologies, bandages or orthopaedic devices were used when necessary, and treatment was only initiated 72 hours after the trauma.
The progression of symptoms was clinically monitored and evaluated by an independent observer using the Steinbroker index modified for athletic activity as follows:
- athletic activity possible without limitations;
- more intensive phases of athletic activity are subject to certain conditions and are limited;
- athletic activity is only possible at a moderate level; the patient is not capable of performing any athletic activity.
In addition, the patients were given a visual analogue scale (VAS) from 0 to 10 where 0 corresponded to no pain upon movement and 10 corresponded to intolerable pain that made the required movements impossible.The evaluation was repeated at the beginning and at the end of the treatment. At the end of the treatment, the patients were also asked for their opinions on the efficacy and tolerability of the therapy.
Results And Discussion
The patients treated were athletes involved in various disciplines: swimming, skiing, football, basketball, volleyball, cycling, and, in particular, running and tennis. The various pathologies treated were subdivided into three groups:
√ Articular involving sprains, effusion, arthrosynovitis, synovitis from overload and from impact, meniscal synovitis, chondropathy, lumbago;
√ Muscular involving 1-3 degree lesions with loss of continuity, myoenthesitis, fibrous scarring;
√ Tendinous involving acute and chronic tendonitis, paratendonitis and entesopathy.
The articular pathologies were represented by 145 cases (44.3%), muscular pathologies by 46 cases (14.1%), and tendinous pathologies by 136 cases (41.5%).
In choosing the pathologies, we considered the indications for diathermy at the short wavelength 4.5 including those for muscular and ligamentary fibrosis, tendinous and articular lesions, bursitis, recurrent inflammation such as traumatic arthritis, and epicondylitis. In regard to contraindications, we referred to general contraindications for application of heat such as infections and sensitivity deficits whereby the patient is unable to perceive or communicate the sensation of possible pain, as well as to contraindications more specific to electromagnetic diathermy such as coagulopathy and thrombophlebitis.
Other examples of contraindications for treatment with short wavelengths such as oedema, articular effusion, and the presence of metallic objects could, instead, be treated with the capacitive energy transfer system in accordance with the builders of the system and some experimental observations2.In this experiment, we treated 12 cases of hydrarthrosis of the knee. In each case, it is necessary to have a correct application of electrodes, respect for time periods, and transmitted energy that must be regulated according to the sensations indicated by the subject in order to avoid causing lesions at the end of the treatment from excessive increases in temperature.
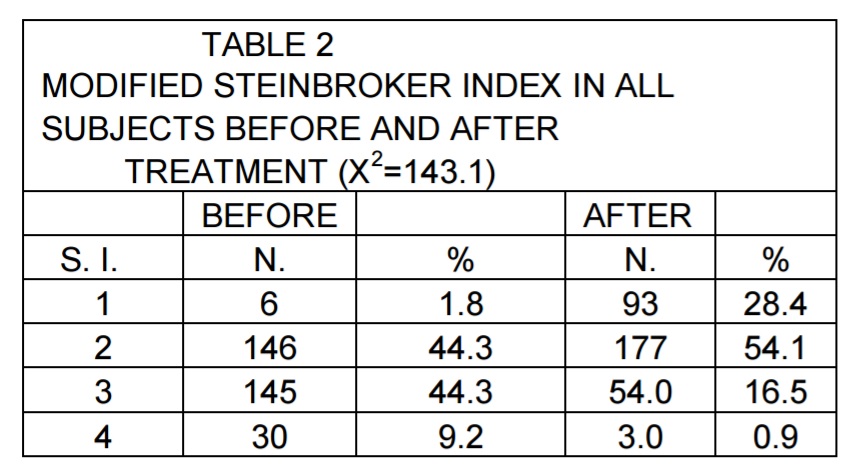
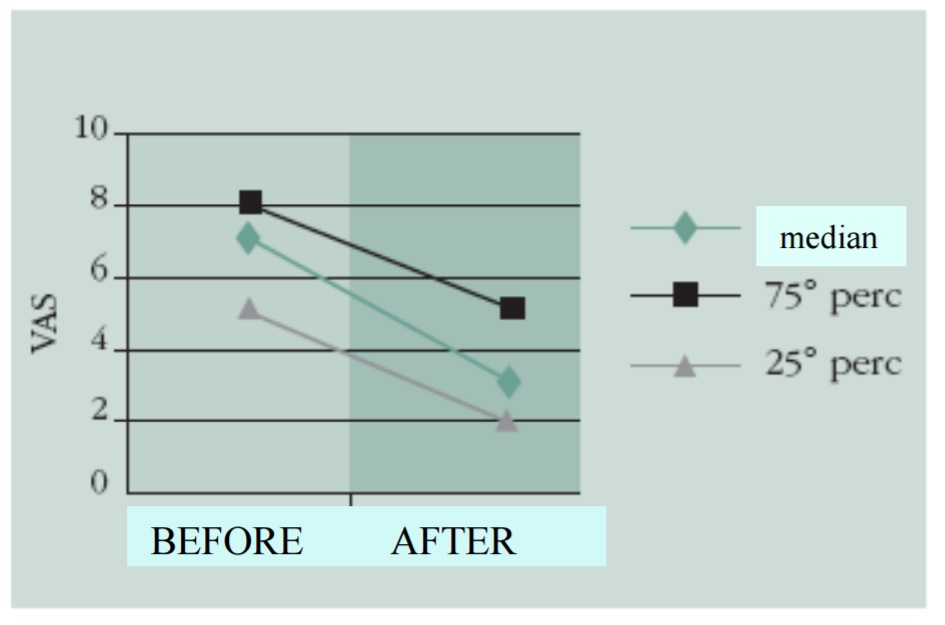
The majority of the patients expressed a reduction in pain and improvement in function at the end of treatment and the categories of the modified Steinbroker index and VAS (Table 2 and Graph 1) were statistically significant.
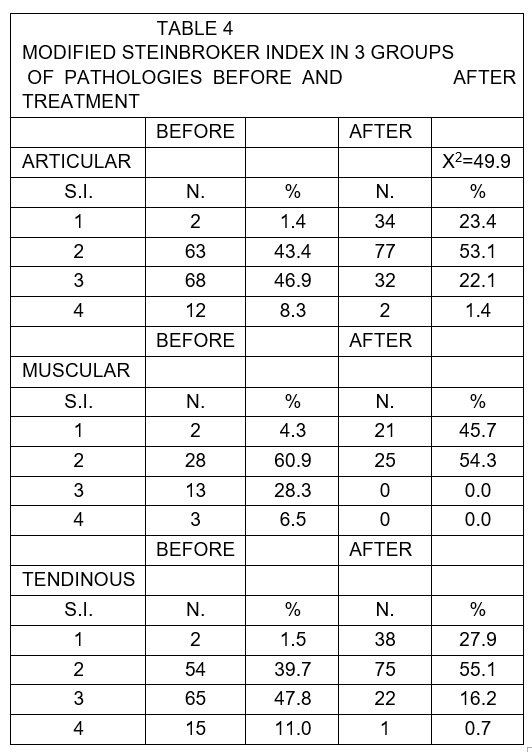
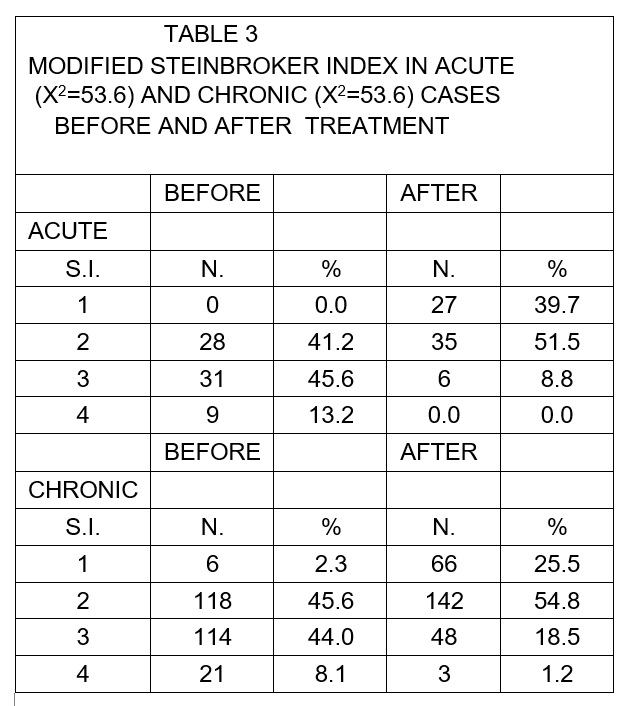
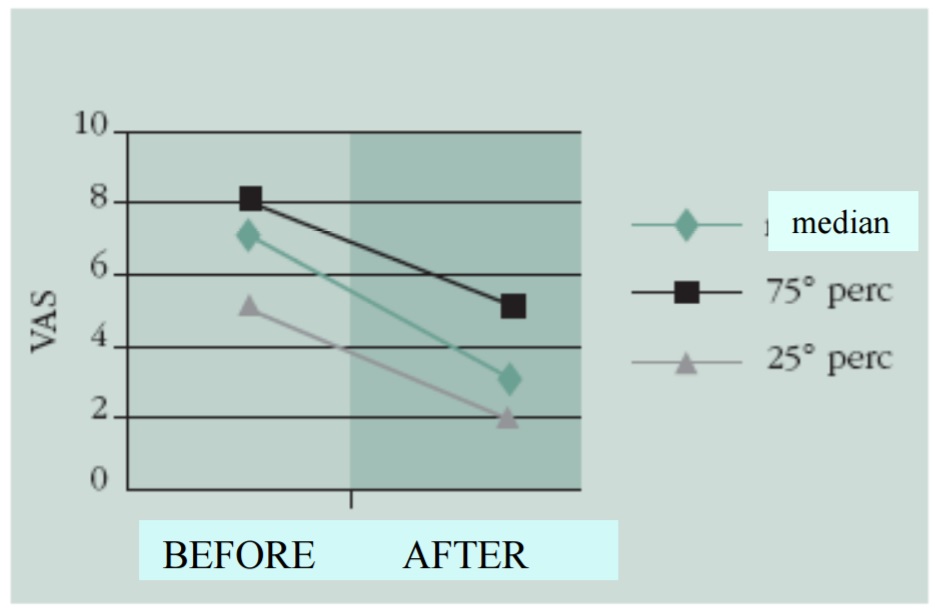
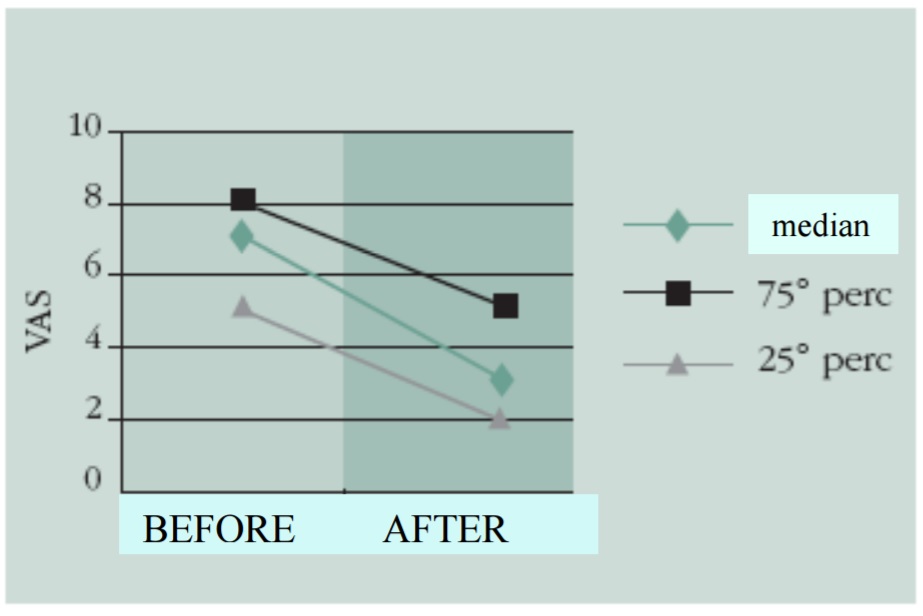
The changes were statistically significant in acute and chronic cases and in the 3 pathology groups observed (Tables 3 and 4 and Graphs 2-6).
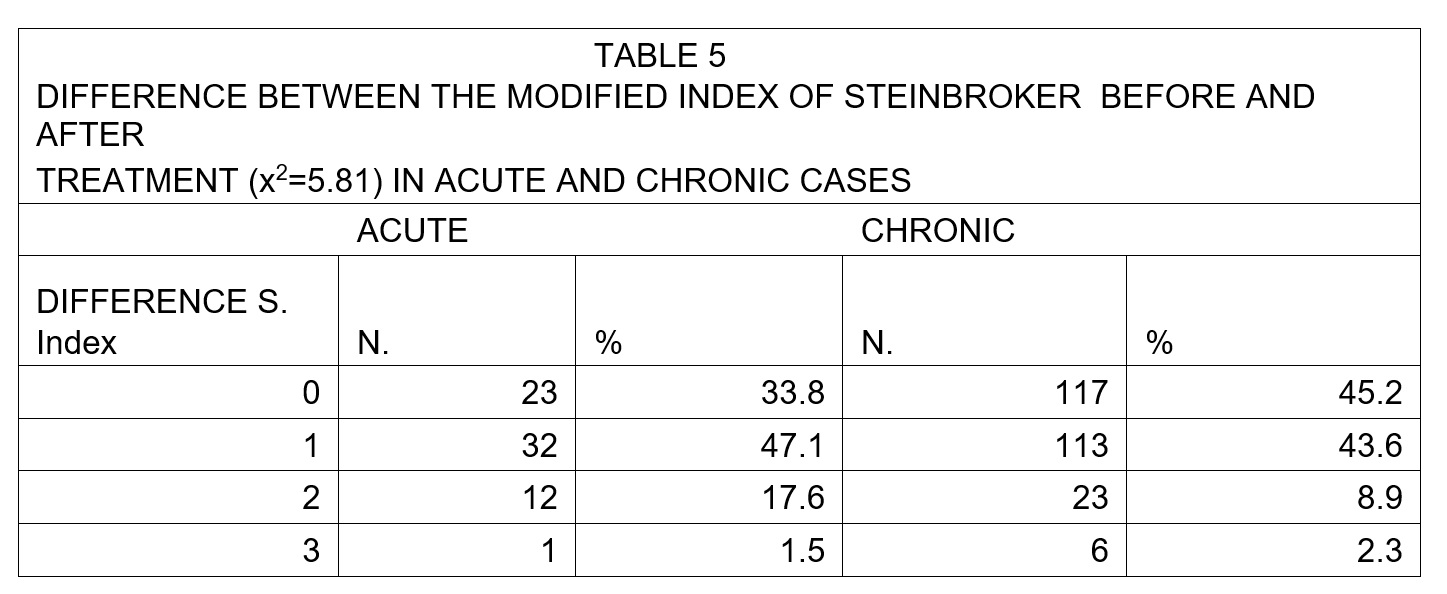
In order to verify the results more thoroughly, we considered the pre-treatment and post-treatment Steinbroker index differences for the various types of pathologies.
In doing so, we were able to observe that in chronic cases (Table 5), 45.2% of the patients did not display changes in functional class and in acute cases, and this figure was 33.8%.
Considering the distribution in all of the classes, however, this difference is not statistically significant, and we must, therefore, state that, statistically, we have not found significant differences between acute and chronic pathologies in terms of reported improvements.
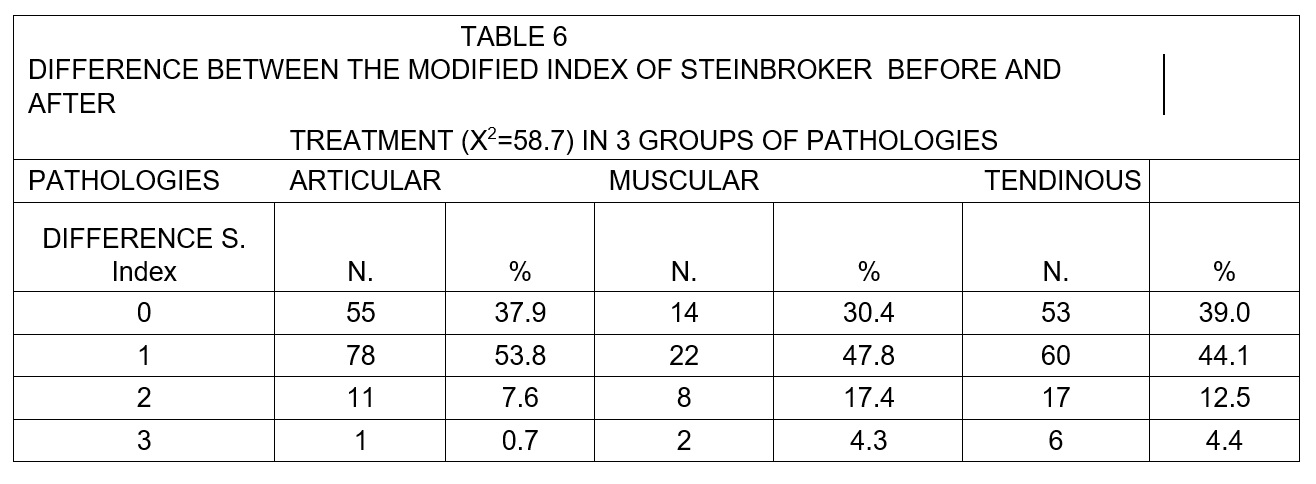
If we consider, instead, the 3 groups of pathologies (Table 6), we are able to observe that the muscular pathologies show a more marked modification in functional class but the patients that remained in the same class before and after treatment represented 30% of the muscular pathology cases and 38-39% of the articular and tendinous cases.
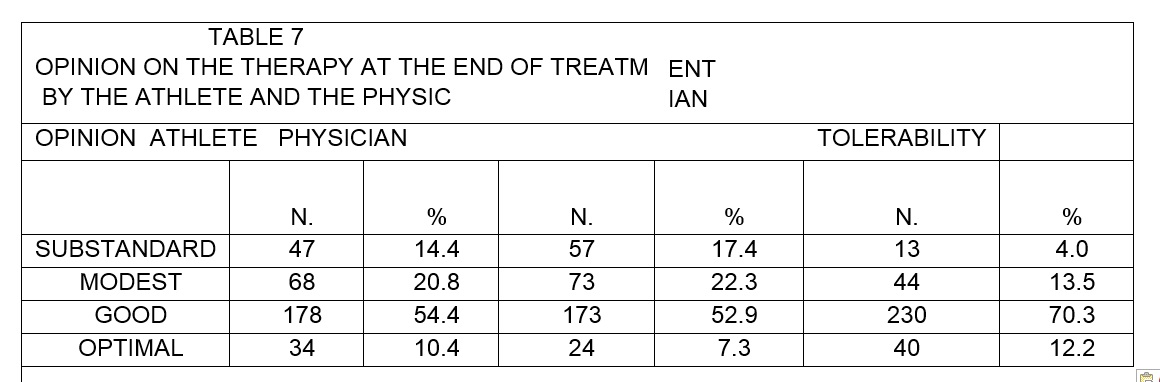
If, instead, we observe the final judgments (Table 7), we see that only 14.4% of the patients report an ineffective treatment without any result. Medical opinion is slightly more severe (17.4%) probably because in some cases the improvement on the basis of the clinical experience was not verified.
Conclusions
The results obtained are interesting and indicate that Tecar® therapy is a useful tool in the treatment of pathologies of the locomotor system in sports. It overlaps with other therapies in terms of the presence or absence of certain positive effects, but it also has distinct characteristics that are effective even where other treatments have failed.
References
- LEVEEN H.H., WAPRICK S., PICONE W.E AL: Tumor eradication by radiofrequency therapy. Response in 21 patients. JAMA 1976; 235:2198-2200.
- LEY A., CLADELLAS J.M., DE LAS HERAS P. E AL: Trasferencia electrica capacitiva (TEC). Tecnica no invasiva de hipertermia profunda en el tratamiento de los gliomas cerebrales. Resultatos preliminaries, Neurochirurgia 1992; 3: 118-123.
- LEHMANN J.F., DE LATEUR B.J.: Therapeutic Heat and Cold, Hydrotherapy. In: Leek J.C., Gershwin M.E., Fowler W.M. Eds. Principles of Physical Medicine and Rehabilitation in the Musculoskeletal Disease. Orlando F1: Grune & Stratton Inc., 1986; 61-101.
- COLE A.J., EAGLESTONE M.A.: The benefits of Deep Heat. Ultrasound and Electromagnetic Diathermy. Physic. Sportsmedicine 1994; 22: 77-88.
- MCMEEKEN J.: Electrotherapy in Zuluaga e al. Eds. Sportphysiotherapy. Applied science & practice. Melbourne: Churcill Livingstone 1995, 233-244.
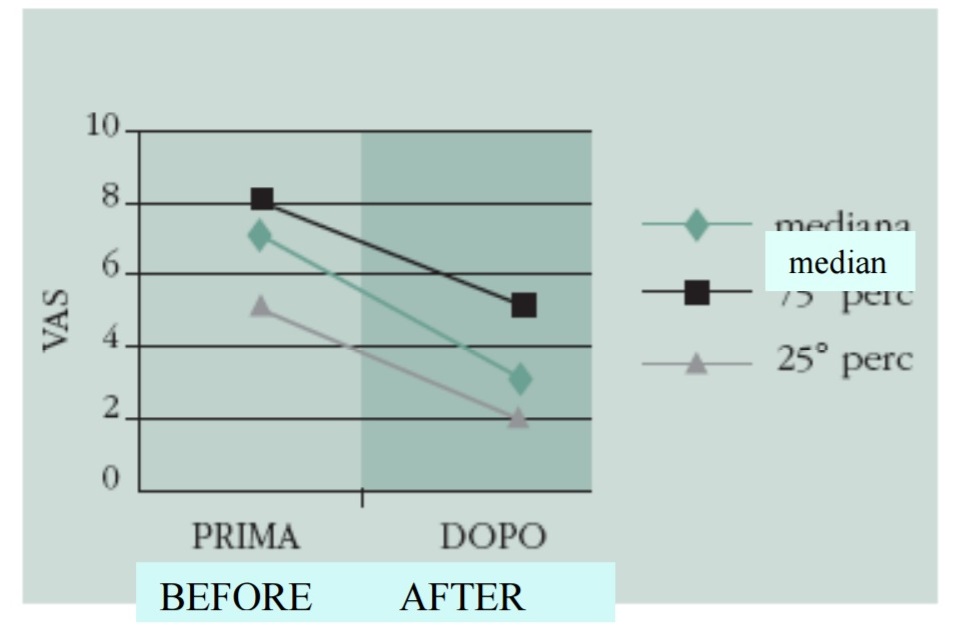
Graph 1. Values of the visual analogue scale of all of the athletes before and after treatment.
Graph 2. Values of the visual analogue scale before and after treatment in cases of acute pathology.
Graph 3. Values of the visual analogue scale before and after treatment in cases of chronic pathology.
Graph 4. Values of the visual analogue scale before and after treatment in cases of articular pathology.
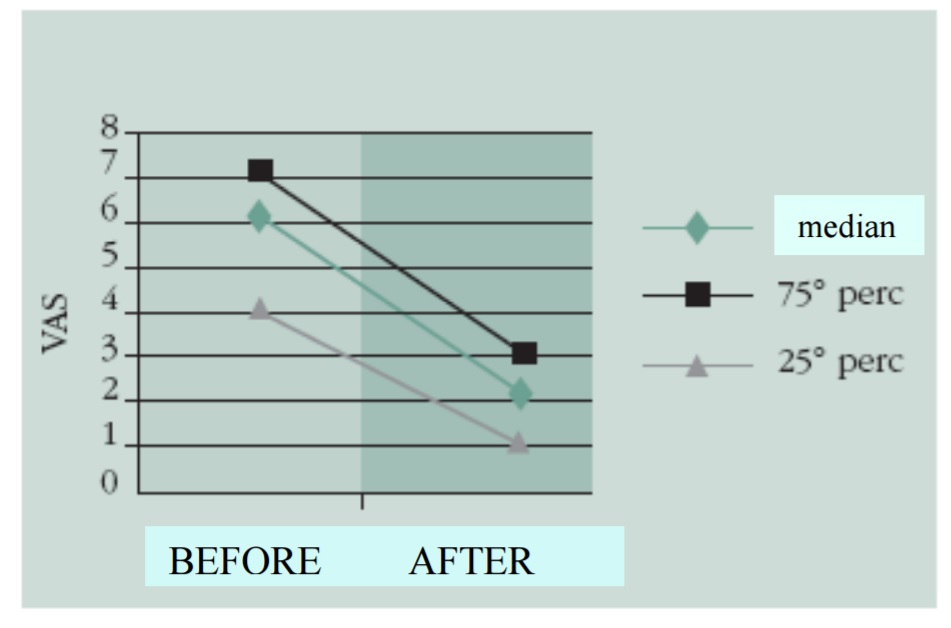
Graph 5. Values of the visual analogue scale before and after treatment in cases of muscular pathology.

Graph 6. Values of the visual analogue scale before and after treatment in cases of tendinous pathology.