 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Tesla
Tesla Nikola
Nikola Kayser
Kayser Fusion
FusionMulticentre study on Tecar Therapy in sports pathologies
- Type: Free
- Download
Multicentre study on Tecar Therapy in sports pathologies
Abstract
This study is a multicentre study conducted on 116 athletes with acute and chronic musculoskeletal and tendinous pathologies, who were administered procedures with TECAR ® therapy, which is a capacitive and/or resistive energy transfer therapy. The objective of the study was to measure the reduction of pain with VAS and to reduce motor recovery time. The experiment was conducted under the management of Professor Carlo Tranquilli in Rome, Gian Paolo Ganzit in Torino, Pasquale Bergamo in Reggio Emilia, and Franco Combi in CInisello Balsamo at Bassini Hospital.
Comprehensive results of some of the groups are reported.
KEYWORDS: Endogenous hyperthermia, musculotendinous trauma, soft tissue pathology
In the treatment of musculotendinous lesions in athletes, the ever-pressing need to strike a balance between the preservation of the individual’s health, the conservation of the societal of the professional athlete, and recovery in the fastest possible time can sometimes exceed all reasonable physiological and clinical considerations, and often puts the physician of high-level sports athletes at the centre of these issues which can seem to be in stark contrast to each other.
In this sense, muscular lesions deserve particular attention, since according to a “traditional” logic, they represent an objective and insurmountable fact that they undoubtedly leave the athlete unfit for a variable period of time. The increasingly frequent attempts at “alternative therapies” often find fertile ground in the needs of the athletes, coaches, and managers that put physicians in a situation in which they have to withstand and share the need to “take care of it quickly”. The possibility of performing physiotherapy treatments in the days after an injury with the hope of speeding up recovery times significantly is certainly a high hope, but this is often just a strong temptation which is not justified by sufficient scientific data.
Recently, TECAR ® therapy (capacitive and/or resistive energy transfer therapy) has been included in the spectrum of possible physiotherapic interventions for early recovery of musculotendinous injuries in high-level athletes. This therapy involves a generator that emits radio frequency signals of 0.5 MHz at a variable power with a maximum of 300 W.
The frequency used is significantly lower than that used in short wave diathermy (27 MHz), in hyperthermy (454 MHz), and in radar therapy (2.5 GHz). Since there is no production of any direct radiation, it must be applied by contact with the body.
By functioning based on a principle that utilizes biological tissue by treating it as electric resistance, or, alternatively, as part of a condenser, this system enables the homogenous involvement of the most external layers as well as the deepest layers of biological tissues.
This possibility is virtually inexistent with irradiating systems in which 30-40% of the supplied energy is already dispersed into the first 10 microns of biological tissue.
For this reason, in order to obtain appreciable results in the deep layers (as in the case of muscular lesions), one is forced to use energy at extremely high frequencies with sizeable limitations in application and problems tied to the strong thermic action produced by the signals.
The TECAR ® system enables the production of an endothermic effect that depends on the applied power and the impedance offered by the tissues upon passage of the current. It is believed that the action depends on the deep endogenous hyperthermia, and, probably on the increase in energy potential of the cellular membranes.
All of the preceding scales are from 0 to 10. 
A series of observations were completed during the last period, on the use of this equipment for the rehabilitation of musculotendinous trauma in high-level athletes. Here, we report the results of these observations carried out simultaneously in various groups at Turin, Milan, Rome, Reggio Emilia which, though still experimental and worthy of more in-depth examination, demonstrate a definite significance in the early treatment of these pathologies.
Case Study Of Group Supervised By C. Tranquilli
25 subjects of both sexes with chronic sports pathologies and between 16 and 35 years of age were treated. All of the subjects were athletes engaging in competitive sports activity, and, in some cases (45%), at an extremely high level (athletes at the national and international level). On average, the athletes participated in 5 training sessions per week. Of these, 18 had acute traumatic pathologies, and 7 had chronic pathologies for which they had already received treatment (by us and by others) with local and general anti- inflammatory therapy, physiokinetic therapy, etc.
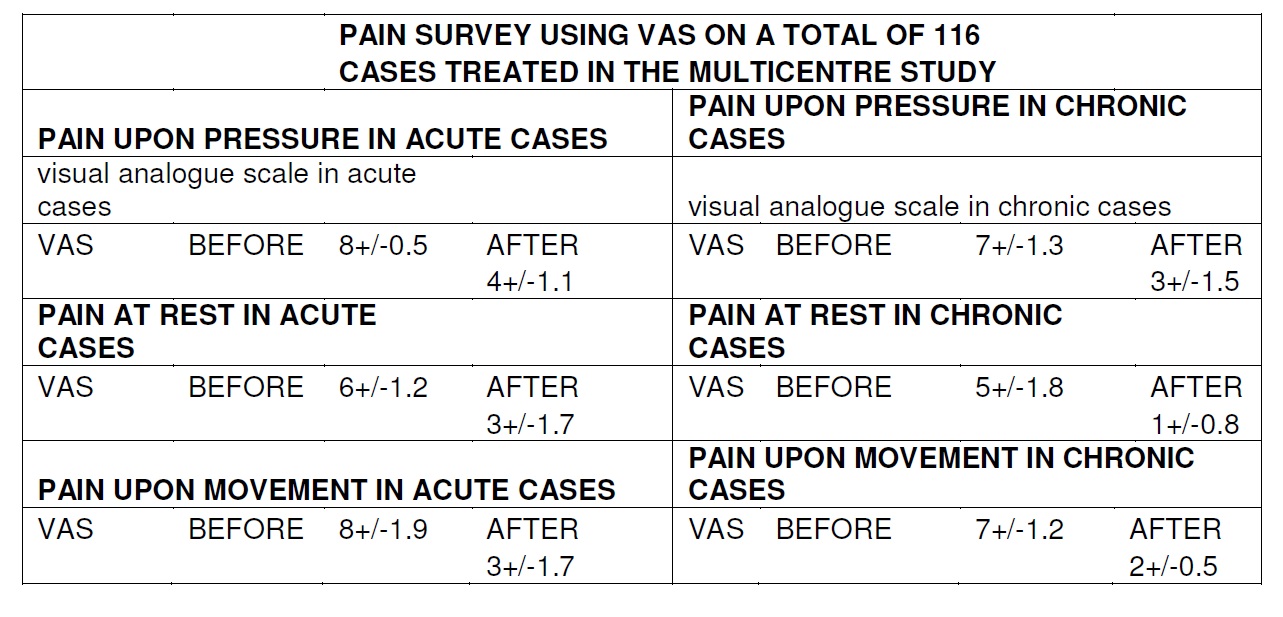
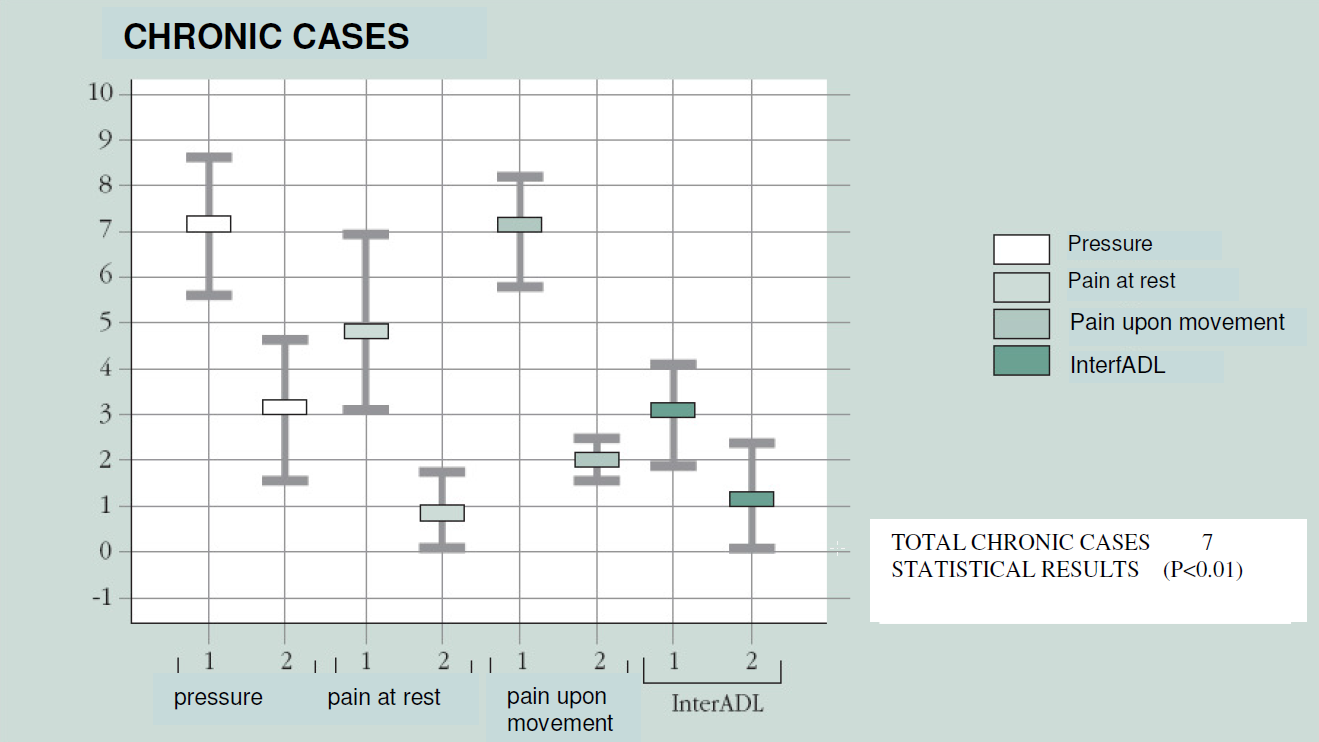
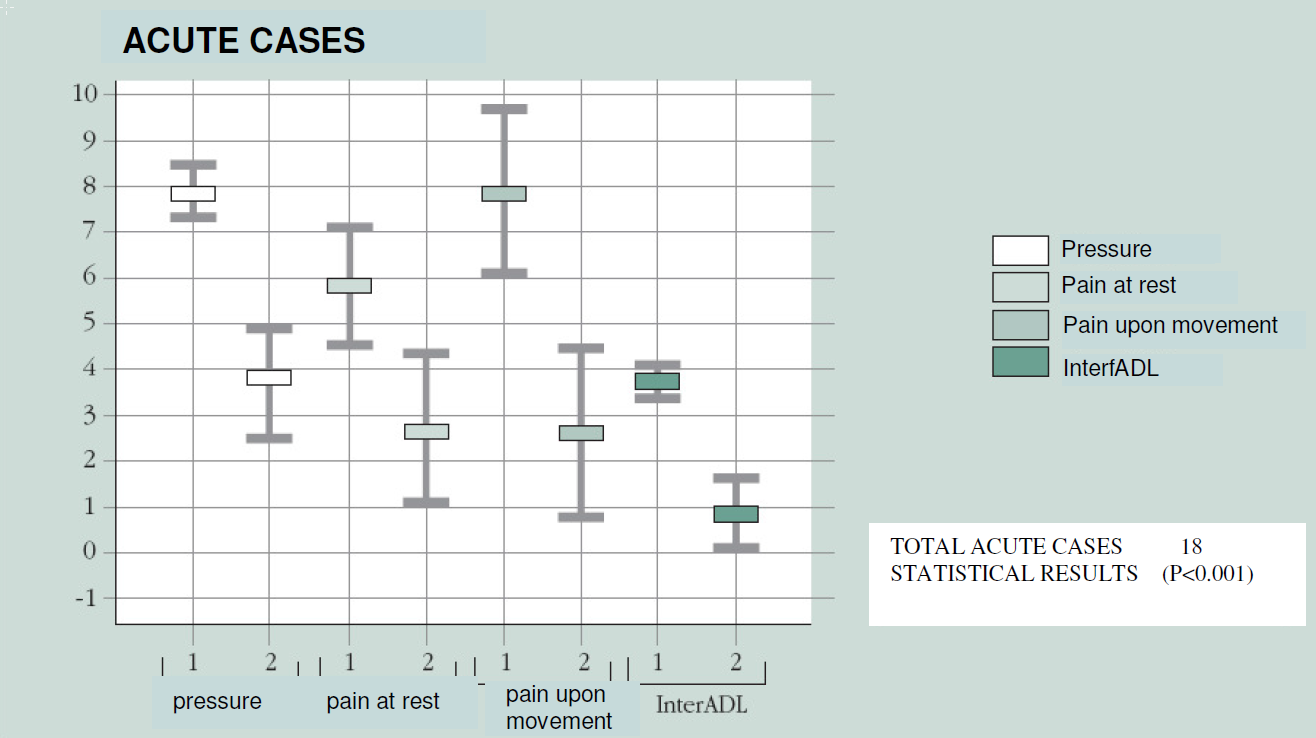
The development of symptoms was monitored by an independent observer using VAS (visual analogue scale) from 0 to 10, in which 0 corresponds to the absence of pain and 10 to the maximum physically perceived pain. The evaluation measured pain upon pressure, at rest, and upon movement. In addition, using a scale from 1 to 4, we evaluated the interference of the pathology with the normal practice of sports (that is, competitive activity consisting of regular training sessions of various frequencies and competitive sports events). The evaluation was performed at the beginning and at the end of the treatment. The data were statistically analyzed with the Student’s t test for paired data.
The results shown in the graphs reveal high statistical significance. This is true for both acute injuries (p<0.001) and chronic injuries (p<0.01). Furthermore, the statistical significance is also high for the analysis of single variables (pain upon pressure, pain at rest, pain upon movement).
With regards to interference with the return to normal sports activity, the majority of the subjects (9 acute and 6 chronic) were able to go back to training sessions relatively quickly compared to normal recovery times for each of the pathologies and, above all, with the absence of relapses and complications.
Only in one case, in a grade II tibiotarsal sprain in a football player, we suspended the treatment temporarily after the first two sessions following increased oedema and hyperaemia. The treatment was continued normally after the fourth day, and after the tenth day from the trauma, the athlete gradually returned to training. 10 sessions were conducted at a daily frequency for all of the patients with acute cases and 15 daily sessions were conducted for chronic cases.
Conclusions
The results showed strong significance in acute as well as chronic injuries with a fast and immediate reduction of the pain and shortened recovery times, determined by a prompt return to activity.
Case Study Of Group Supervised By P. Bergamo
In the football season of 1996/97, we adopted a new method of energy transfer for traumatic acute pathologies of soft tissues. There were 12 subjects, all professional football players of A. C. Reggiana, presenting:
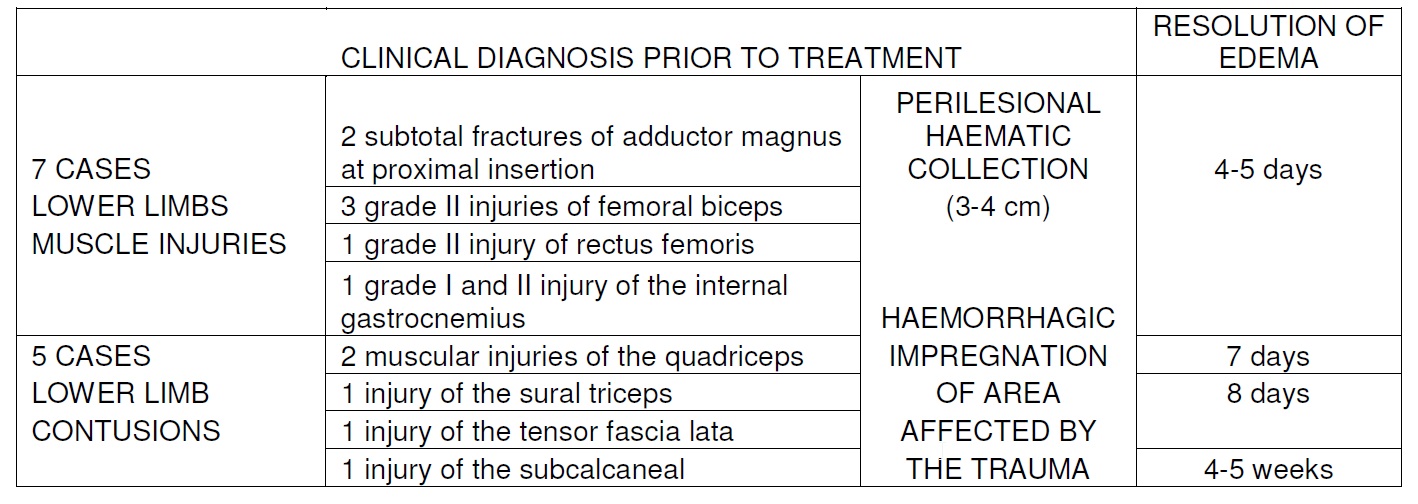
√5 contusions of the lower limbs (4 were muscular, and of these, 1 was of the quadriceps, 1 of the sural triceps, 1 of the tensor fascia lata, and 1 of the subcalcaneal).
√7 injuries to the lower limbs (2 subtotal fractures of the adductor magnus at the proximal insertion, 3 grade II injuries of the long head of the femoral biceps, grade II injury of the rectus femoris, and grade I-II injury of the internal gastrocnemius).
The clinical diagnosis was confirmed by diagnostic examination via an initial ultrasound and subsequent daily ultrasound monitoring personally performed in our outpatient clinic, which has the required equipment. In all of the injuries, there was a haemorrhagic imbibition of the area affected by the trauma in the tearing of the adductor, and in particular, there were consistent perilesional haematic masses (3-4 cm in diameter).
For all of the subjects, the therapy started in the acute phase included: for the first 5- 6 days, 2 sessions of 30-35 minutes per day until pain symptoms were resolved. In the treated contusive traumas, which produced immediate functional impotence (excluding subcalcaneal trauma, which required a longer period of time, 4-5 weeks), the resolution of oedema and pain symptoms was notably influenced as the 2 athletes affected by contusive trauma of the quadriceps went back to competitive sports activity after 7 days, and the other 2 who suffered from the same pathology of the sural triceps and tensor fascia lata returned to regular training after 8-9 days.
For major muscular injuries to the adductor muscles, it was verified and registered with daily ecographic documentation that there was a progressive and rapid reabsorption of haematic effusion in both at the end of the first week of treatment.No phenomena of bone calcium aggregation of haematic deposits was observed.
Also, the oedema around the injury (peri-tissular fill-in or impregnation that is normally observed in ultrasound examinations as early-onset hyperecogenic area) observed in the other muscle injuries, developed in 4-5 days with complete and total reabsorption.
Considerations
The preliminary results of this study are the results of clinical, diagnostic, and reeducative daily checks in the field. Certainly, it can be affirmed that this equipment produces an energy transfer to the soft tissues, which is capable of improving membrane exchanges, inducing the drainage of blood and serum effusion, despite the use of heat. We were rather skeptical and hesitant to adopt this method in the acute phase and, especially, in richly vascularised tissues. Nevertheless, it is precisely in these anatomical locations where we found the most outstanding effect in terms of resolution.
In fact, the only case which did not display a significant improvement was the subcalcaneal trauma, which is an area with notoriously little vascularisation.
Conclusions
Though modern research methods have led to a safe interpretation of trauma of the soft tissues, current therapeutic support still does not have equipment and methodology capable of quickly resolving even simple muscular trauma, in a world of Italian professional football that is becoming increasingly frustrated.
In our opinion, this equipment is valid for an adequate and fast resolution of oedema and of its potentially resulting serum and blood accumulations. It is well-accepted by our demanding patients,who in the majority of cases, already report beneficial effects with regard to pain and functional limitation as early as after the first sessions.
Certainly, fast recovery of this stage (resolution of reflexive painful contractions; bringing together the stumps of the injury) is a fertile ground for the subsequent scarring phase, creating the essential requirements for a complete, safe healing of the injury.
We underline “complete and safe” and not “fast and miraculous” since it is wellknown by those of us who work with these pathologies how uncertain and dangerous it is to search for records with suggestive and, sometimes, invasive methods, rather than physiological methods through treatments without side effects,which would be the right means for proper rehabilitation both in the gym and on the pitch.
Case Study Of Group Supervised By F. Combi
41 subjects of both sexes between 20 to 60 years of age were divided into acute and chronic pathologies and treated. 33 cases were acute, and 8 cases were chronic and had received various periodic treatments.
As Follows :
no. 1 Achilles tendon tendinitis
no. 3 sural biceps injury
no. 3 medial gemellus insertion
no. 2 rectus and oblique tendinosis
no. 2 patellar ligament tendonitis
no. 2 tarsal tendon trauma
no. 4 femoral biceps injury
no. 2 medial epicondylitis
no. 2 shoulder contusion
no. 1 adductor cruralgia
no. 1 quadriceps injury
no. 1 rectus femoris injury
no. 2 adductor tendinitis 1st finger, metacarpal tunnel tendinitis
no. 1 LS-S1 joint pain
no. 3 osteoarthritis of the spine
no. 2 bilateral osteoarthritis
no. 2 osteoarthritis of the hip
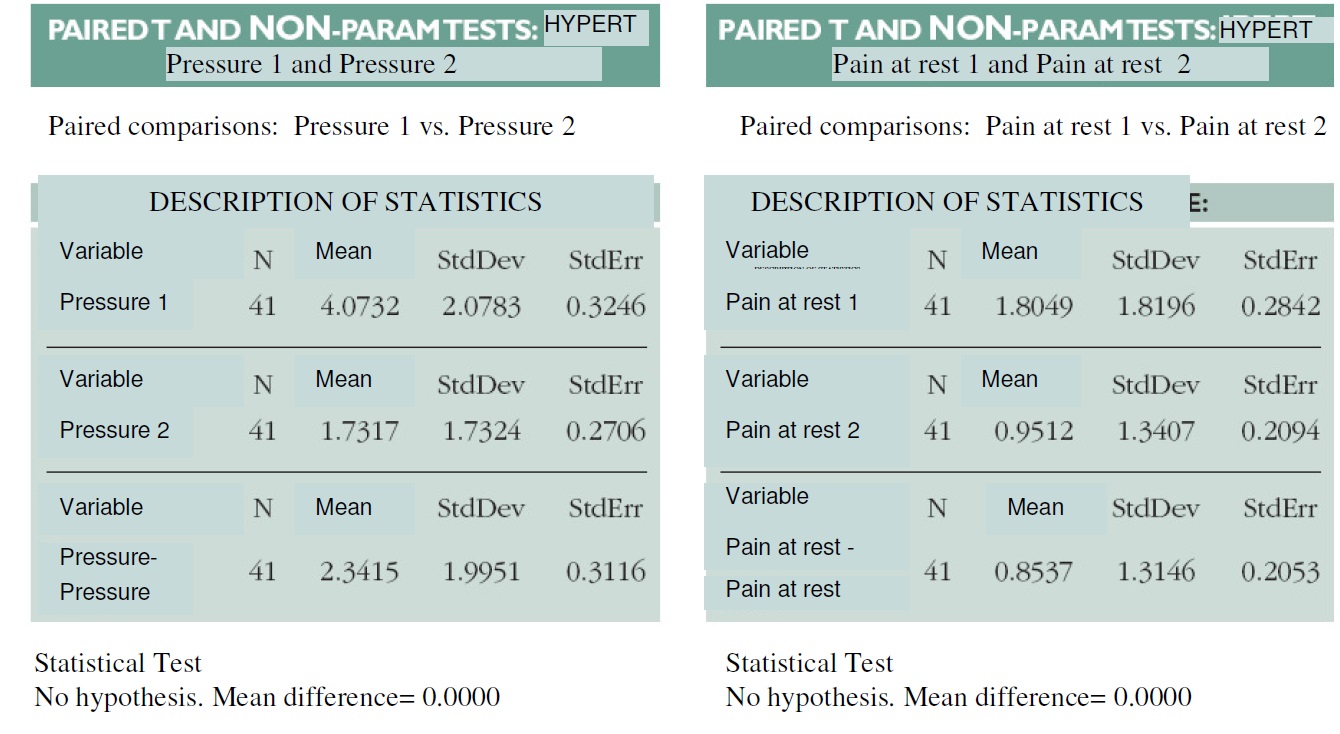
The development of symptoms was monitored with a visual scale from 0 to 10 in which 0 corresponds to the absence of pain upon pressure, at movement, and at rest, and 10 corresponds to maximum pain upon pressure, at movement, and at rest.
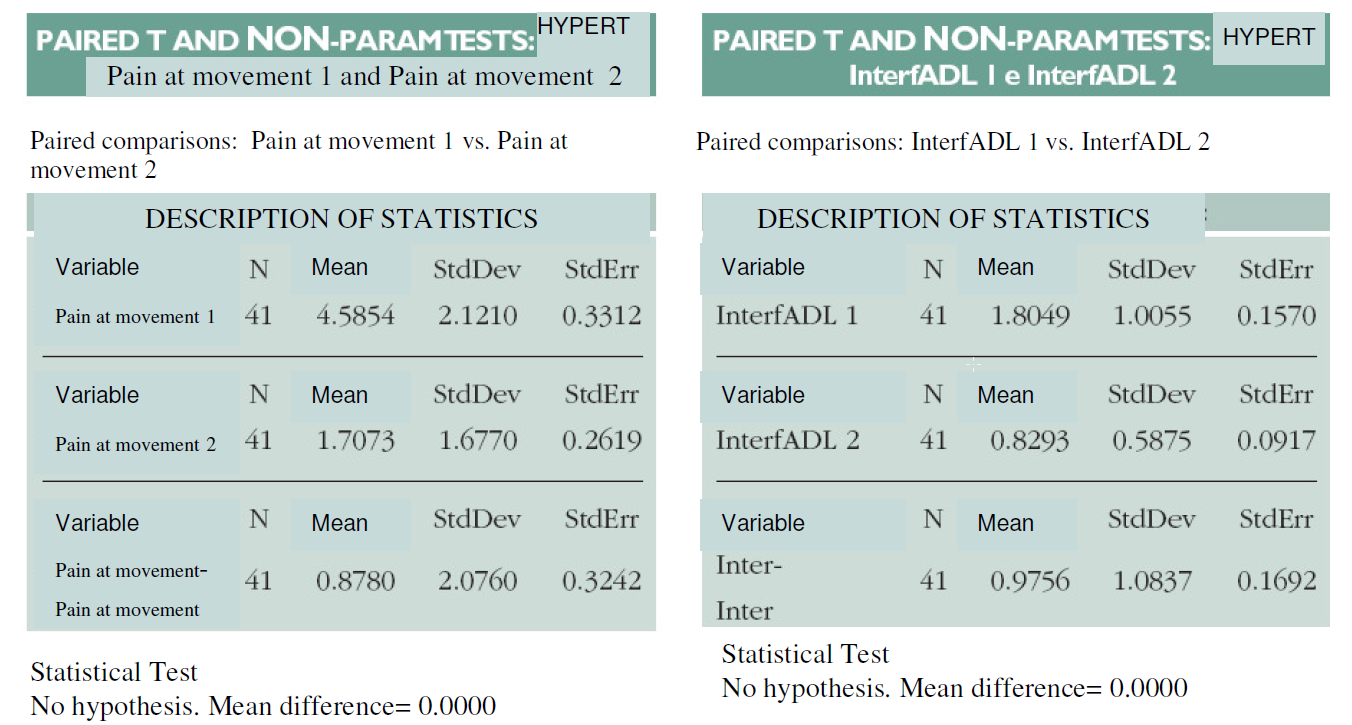
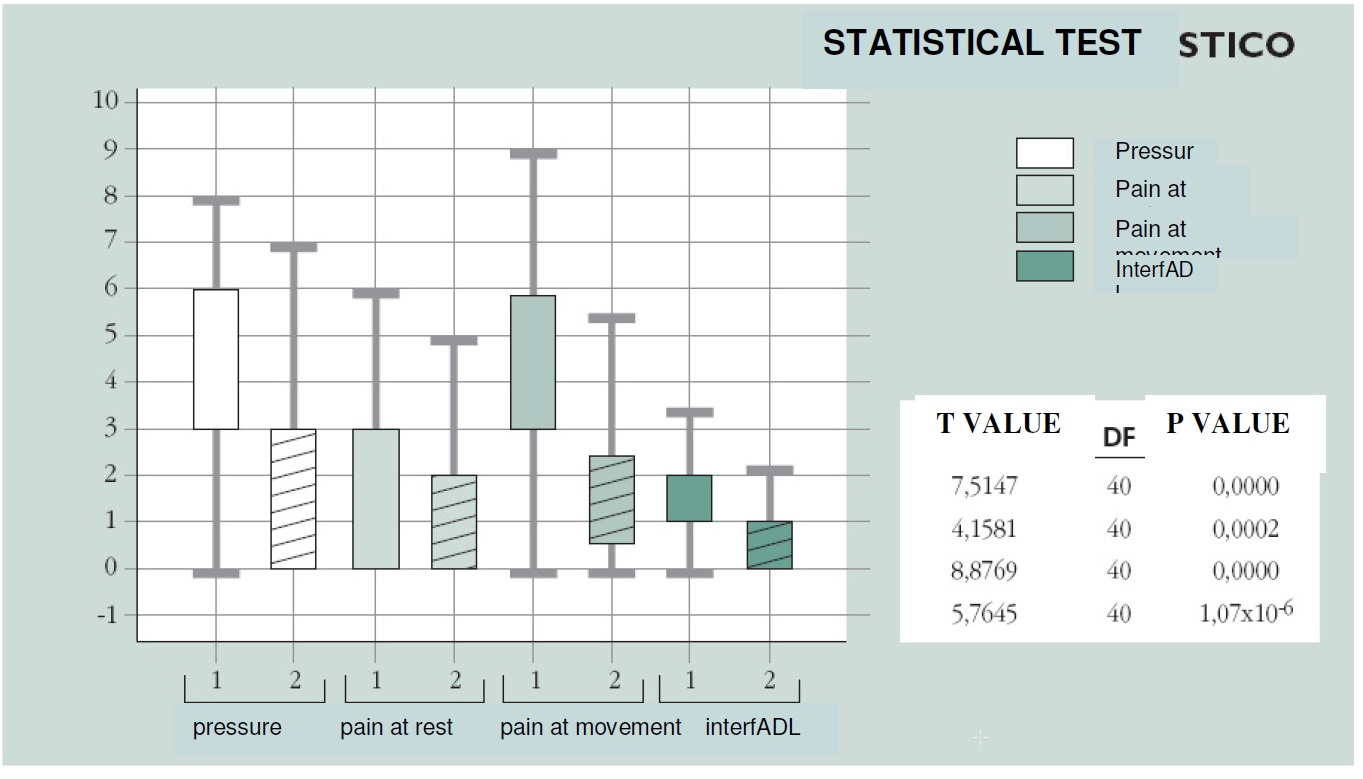
We used a scale from 1 to 4 to evaluate the interference with daily routine. We indicated the pre-treatment pain symptoms with pressure 1, movement 1, and rest 1, and we indicated the post-treatment pain symptoms with pressure 2, movement 2, and rest 2. The evaluation was performed through statistical processing of the data. As can be seen from the tables and graphs on the following page, the majority of the subjects reported a considerable improvement of pain upon pressure, at rest, and during movement, in addition to a return to normal daily living.
The statistical processing of data results in a P value of <0.001 in cases of muscular lesions. In 4 cases of muscular lesions (2 lesions of the medial gemellus, 1 of the rectus femoris, and 1 of the femoral biceps), muscle ultrasound was performed before and after the treatment. The ultrasound scans showed a reduction in the diameter of the lesions.


Refrences
1. COLO A.J., EAGLESTONE M.A.: The benefits of deep heat. Ultrasound and Electromagnetic Diathermy. Physic Sportsmedicine 1994; 22: 77-88
2. GRIBAUDO C.G., ASTEGIANO P, CANALA GL, GANZIT GP: Trattamento con ipertermia a trasferimento energetico resistivo e capacitivo di lesioni muscolo scheletriche acute e croniche: risulatati preliminari in “Radiazioni in medicina: qualitá e sicurezza.” Atti del Congresso –Fisica Sanitaria- n. 1/97 gennaio/marzo; 379-381
3. MCMEEKEN J.: Electrotherapy in “Zuluaga et al. Eds Sportphysiotherapy, Applied Science & practice”. Melbourne: Churcill Livingstone 1995, 233-244
4. LEY A., CLADELLAS J.M., DE LAS HERAS P. ET AL.: Trasferencia Electrica capacitiva (TEC). Técnica no invasiva de Hypertermia profunda en el tratamiento de los gliomas cerebrales. Resultados preliminares. Neurochirurgia 1992; 3ç:118-123





