Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Tesla
Tesla Nikola
Nikola Kayser
Kayser Fusion
FusionExtracorporeal shock wave therapy and how to treat frozen shoulder
- Type: Free
Extracorporeal Shockwave Therapy As an Adjunctive Therapy for Frozen Shoulder
A Systematic Review and Meta-analysis
Ruihan Zhang,* MMed, Zhenyu Wang,*† MD, Ruishu Liu‡ MMed, Nan Zhang,* MMed, Jiaxun Guo,* MMed, and Yunxia Huang,* MMed
Investigation performed at Yongchuan Hospital, Chongqing Medical University, Chongqing, China
Background: The best nonsurgical treatment for frozen shoulder is still unclear. Extracorporeal shockwave therapy (ESWT) is an innovative adjunctive treatment for frozen shoulder, but its effect is still unclear.
Purpose: To evaluate the published literature regarding the potential of ESWT as an adjunctive therapy for frozen shoulder.
Study Design: Systematic review; Level of evidence, 1.
Methods: Searches were conducted in the PubMed, EMBASE, Cochrane Library, China National Knowledge Infrastructure (CNKI), and VIP Information databases for relevant studies between inception and November 2020. Included were randomized controlled trials (RCTs) for frozen shoulder that compared ESWT with routine treatments to controls. There were no restrictions on the treatment period, type of ESWT, or severity of symptoms. At least 1 of the following outcome indices was assessed: visual analog scale (VAS) for pain, Constant-Murley score (CMS) for shoulder function assessment, or external rotation range of movement (ER ROM). RevMan 5.3 software was used to evaluate the bias and quality of the included studies. For continuous variables, the mean difference (MD) or standardized MD (SMD) with the 95% CI was extracted. For dichotomous data, event ratios and sample sizes were extracted.
Results: Overall, 20 studies were included. The ESWT used as an adjunct to other interventions had better outcomes compared with control groups regarding immediate and short-term analgesic effects (immediate: MD, –1.10 [95% CI, –1.27 to –0.92], P < .00001; short-term: MD, –0.72 [95% CI, –0.94 to –0.50], P < .00001) as well as immediate function (SMD, 1.54 [95% CI, 1.19 to
1.89], P < .00001], I2 ¼ 0%). There was significant heterogeneity between studies for long-term analgesia (MD, –0.90 [95% CI,
–1.40 to –0.41], P < .00001, I2 ¼ 89%) and ER ROM (MD, 10.31 [95% CI, 3.46 to 17.17], P < .003, I2 ¼ 93%).
Conclusion: ESWT seems to be beneficial to patients with frozen shoulder by alleviating pain and improving function. ESWT could be used as an adjunct therapy to routine treatments, although the quality of the included RCTs was hampered by significant heterogeneity regarding long-term analgesia and joint ROM.
Keywords: extracorporeal shockwave therapy; frozen shoulder; pain; motor function; meta-analysis
Frozen shoulder is a common musculoskeletal disorder characterized by pain, limited joint mobility, and dysfunction,18 with prevalence rates ranging from <1% to 2%.19
Frozen shoulder is clinically divided into 3 overlapping phases. The painful freezing phase has a duration of 10 to
36 weeks and is characterized by pain and stiffness around the shoulder, which may worsen at night. The adhesive phase is characterized by restricted range of movement (ROM) with a gradual relief of pain, which occurs at 4 to
12 months. The resolution phase with spontaneous improvement in the ROM takes 12 to 42 months.7 Frozen shoulder is a self-limited condition, but the recovery may be
The Orthopedic Journal of Sports Medicine, 10(2), 23259671211062222
DOI: 10.1177/23259671211062222 The Author(s) 2022
Slow and incomplete, which reduces patients’ activities of daily living and increases their medical burden.18, 26
Because of the uncertainty of the efficacy and risk of surgical treatment, nonsurgical treatments are more likely chosen by patients.2,17 Among them, intraarticular steroid injection and physical therapy are commonly used nonsurgical treatments and have shown some benefits.27,40 However, because the 3 stages of frozen shoulder often overlap and the clinical symptoms of patients are complex, adjuvant therapy is often needed throughout the course of treatment. Zhang et al 40 and Dias et al 7 identified that the benefits of steroid injection were specific to the painful freezing phase and not to the adhesive phase of frozen shoulder. Physical therapy provides more obvious benefits in the adhesive phase than in the painful freezing phase.40
This open-access article is published and distributed under the Creative Commons Attribution Noncommercial - No Derivatives License (https://creativecommons.org/ licenses/by-nc-nd/4.0/), which permits the noncommercial use, distribution, and reproduction of the article in any medium, provided the original author and source are credited. You may not alter, transform, or build upon this article without the permission of the Author(s). For article reuse guidelines, please visit SAGE’s website at http://www.sagepub.com/journals-permissions.
In recent years, extracorporeal shockwave therapy (ESWT) has been increasingly used as an adjunct to other interventions in some randomized controlled trials (RCTs) and has shown satisfactory improvement in multiple aspects.3,13,30 To date, there is no specialized meta- analysis or systematic review evaluating the effectiveness of ESWT as an adjunctive therapy in treating frozen shoulder. Therefore, the purpose of this study was to perform a
Meta-analysis to evaluate the effectiveness of ESWT as adjunctive therapy for frozen shoulder. We hypothesized that ESWT would be a positive adjunctive therapy in the treatment of frozen shoulder.
METHODS Search Strategy
A comprehensive search utilizing Preferred Reporting Items for Systematic Reviews and Meta-Analyses guide- lines was performed via PubMed, EMBASE, Cochrane Library, China National Knowledge Infrastructure (CNKI), and VIP Information databases between inception and November 2020. The medical subject headings/key- words were “extracorporeal shockwave therapy,” “frozen shoulder,” “randomized controlled trial,” and “meta-analysis.” Variations of different terms were used to make a systematic search. The complete search strategy used in PubMed is shown in Appendix Table A1. The reference lists of relevant reviews and registered trials were also reviewed to ensure completeness of the search.
Inclusion Criteria
The inclusion criteria were as follows: (1) RCTs; (2) patients who were diagnosed with frozen shoulder and were experiencing pain and restricted joint movement; (3) the experimental groups were treated with ESWT plus routine treatments, the control groups were treated with routine treatments, and the routine treatments were the same in both groups; (4) there were no restrictions on the treatment period, type of ESWT, or severity of symptoms, and the energy intensity was dependent on the tolerance of the patient; (5) the languages were limited to Chinese and English; (6) whether or not to adopt a blinded method was unlimited; and (7) the authors used at least 1 of the following outcome indices: visual analog scale (VAS), Constant Murley score (CMS), and external rotation ROM (ER ROM).
Exclusion Criteria
The exclusion criteria were as follows: (1) patients experiencing the following comorbidities: rotator cuff disease, fractures, calcifying tendinitis, glen ohumeral arthrosis, my official pain syndrome, or other diseases that can cause shoulder pain and dysfunction; (2) the original data were not suitable for a meta-analysis, and it was impossible to obtain usable data by contacting the authors; and (3) different types of ESWT were compared with each other.
Data Extraction
Two reviewers (N.Z., J.G.) Independently screened the titles and abstracts according to the inclusion and exclusion criteria and thoroughly read the full texts of relevant literature. Studies that met the predefined criteria were included. In the case of a disagreement, a third reviewer (Z.W.) was consulted to assist in the assessment.
Another 2 reviewers (R.L., Y.H.) independently extracted the following data: first author, publication year, sample size, intervention details, follow up (where avail- able), measurement time, and outcome indices.
Pain intensity was assessed via the VAS (the lower the score, the better the effectiveness). Shoulder function was assessed via CMS (the higher the score, the better the function). The joint ROM was assessed via ER ROM (the higher the degree, the better the curative effect).
The period of assessment was artificially defined as follows: immediate, short-term (<3 months), and long-term ( 3 months).The results at multiple follow-up times from the same study were included in the subgroup analyses by time point. When 2 studies used the same group of participants, the 2 studies were included only when different out- come measures were used.
Bias Assessment and Quality Classification
We evaluated the quality of the included studies using the Cochrane Collaboration’s tool for assessing risk of bias in randomized trials,11 using RevMan version 5.3 (Nordic Cochrane Centre, The Cochrane Collaboration).
Statistical Processing and Assessment of Heterogeneity
For continuous variables, the mean difference (MD) or standardized MD (SMD) with the 95% CI was extracted. For dichotomous data, event ratios and sample sizes were extracted. Throughout the analyses, a 2-sided test was
†Address correspondence to Zhenyu Wang, MD, Department of Rehabilitation Medicine, Yongchuan Hospital, Chongqing Medical University, Chongqing, 402160, China (email: This email address is being protected from spambots. You need JavaScript enabled to view it.
*Department of Rehabilitation Medicine, Yongchuan Hospital, Chongqing Medical University, Chongqing, China.
‡Department of Dermatology, Yongchuan Hospital, Chongqing Medical University, Chongqing, China. Final revision submitted August 3, 2021; accepted September 3, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by funds from the
National Natural Science Foundation of China (NSFC No. 81674066); the Natural Science Foundation of Chongqing Province (No. cstc2017jcyjAX0397); the
TCM Foundation of Chongqing Health Committee of China (No. zy201602119); and the Science Foundation, Yongchuan Hospital of Chongqing Medical University (No. YJYJ201603). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
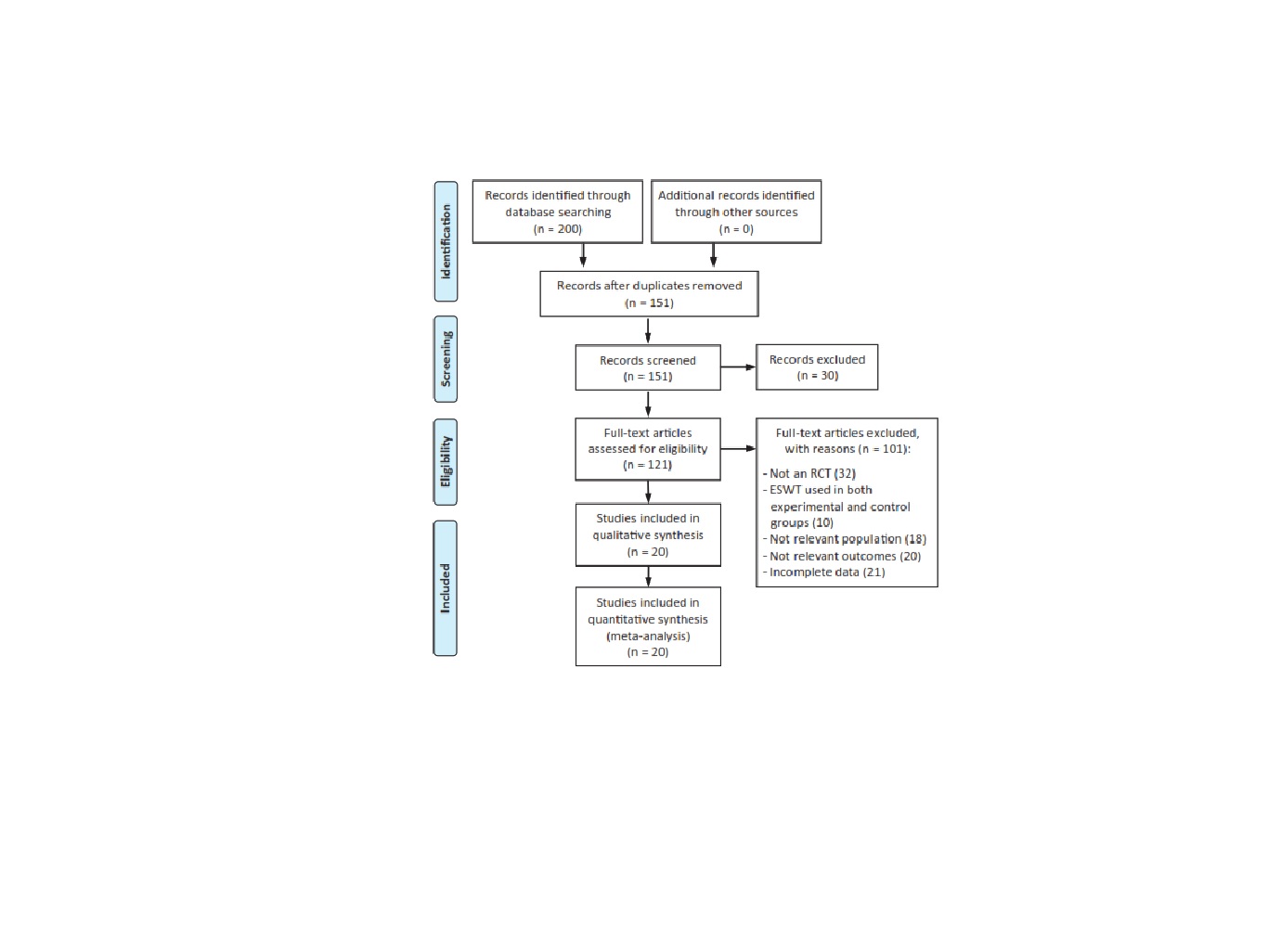
Figure 1. Study flow diagram. ESWT, extracorporeal shockwave therapy; RCT, randomized controlled trial
Used, and P values .05 were considered to be statistically significant.
Heterogeneity was evaluated by using the I2 statistic and
The Cochran Q statistic with P values.26 the data were pooled using the random-effects model if significant hetero-
Study Characteristics
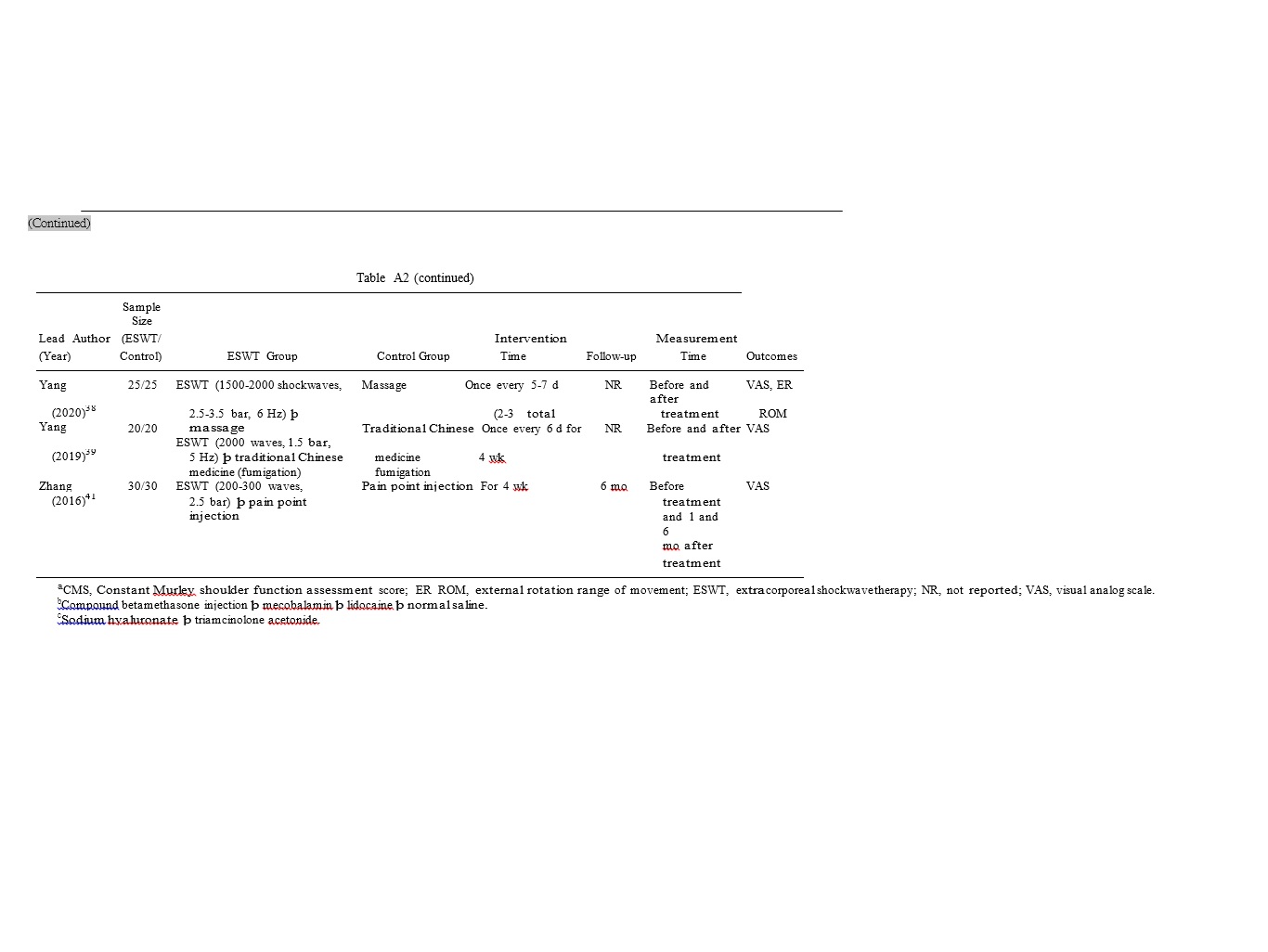
The characteristics of the included studies are listed in Appendix Table A2. Patients in the adhesive phase were identified in 18 studies,kand patients in the remaining,
Geneitywas present (I2 > 50% or PQ < .1); otherwise, a
2 studies
Were in the overlap of the painful freezing
Fixed effects model was used. In the case of significant het- erogeneity, subgroup analyses were further conducted to investigate the potential source of heterogeneity on the treatment effect size.11 the statistical software used was Rev Man 5.3 software. A descriptive analysis was performed if data could not be combined.
RESULTS
Study Selection
Initially, 200 records were identified via the electronic database search. Of these, we evaluated 121 full texts for eligibility. Ultimately, 20 RCTs§ were included in this review. The flow diagram of the selection process is shown in Figure 1.
Phase and adhesive phase. Two1,8 of the included studies
Were3-arm studies, and appropriate data were selected for the statistical analysis based on the inclusion and exclusion criteria.
Methodological Quality and the Risk of Bias Within Studies
The risk of bias graph and the risk of bias summary are shown in Figure 2. Of the included studies, 18{ utilized a suitable method to minimize bias and were considered to have a low risk of selection bias, performance bias, detection bias, attrition bias, reporting bias, and other biases. One24 of the included studies had a high risk of bias in the randomization scheme, and one36 of the included studies had a high risk of other biases.
- References 1, 4-6, 8, 9, 12, 20, 24, 25, 29, 31-34, 36-39, 41.
kReferences 1, 4-6, 9, 12, 20, 24, 25, 29, 31-33, 36-39, 41.
{References 1, 4-6, 8, 9, 12, 20, 25, 29, 31-34, 37-39, 41.
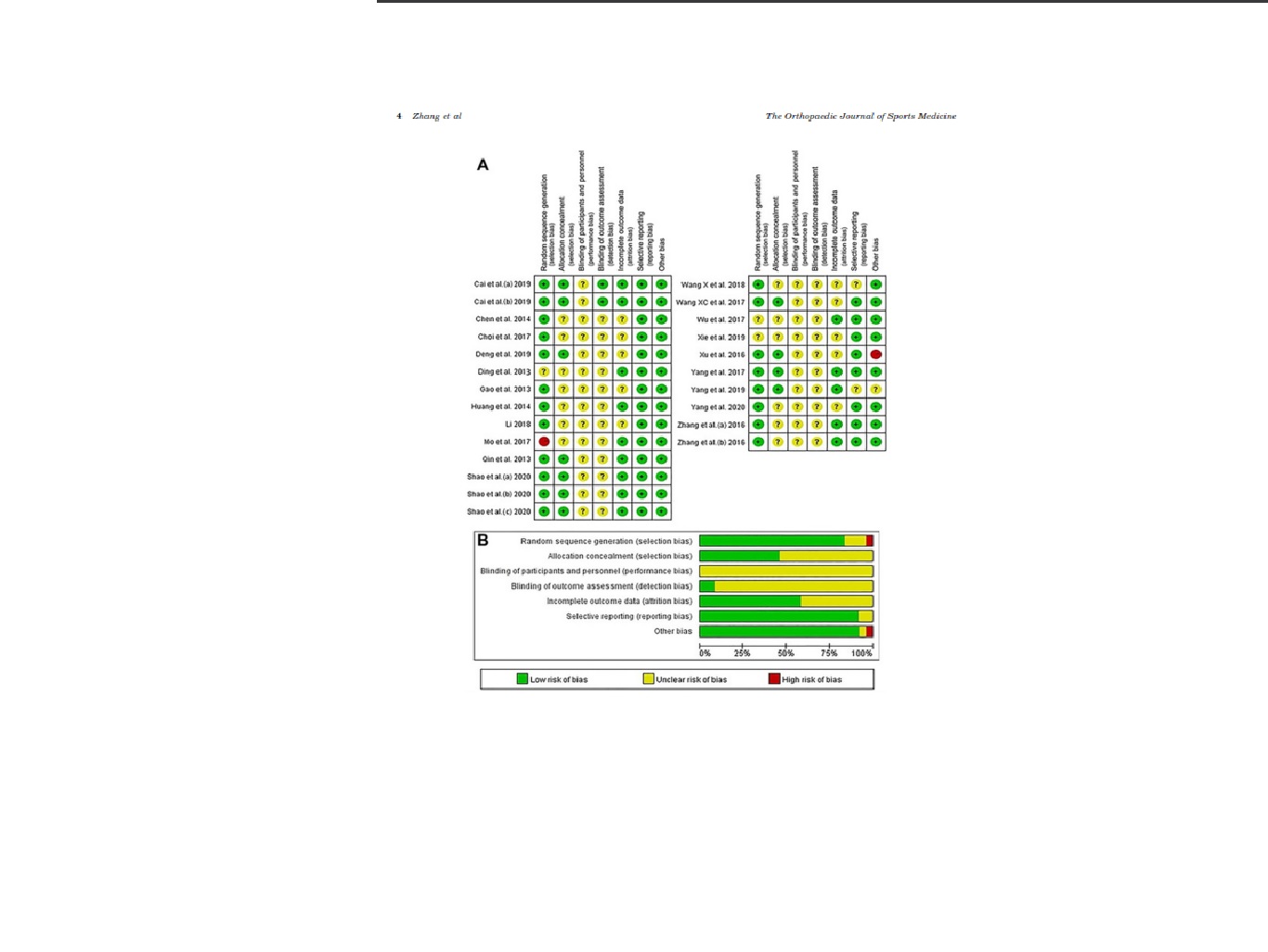
Figure 2. Risk of bias (A) table and (B) summary. a, sodium hyaluronate þ triamcinolone acetonide. Within the figure the three time points were marked as a, b and c, and relate to before treatment, immediately after treatment and 3 months after treatment.
Pain Intensity
Overall, 18 studies# assessed the post intervention effective- ness of ESWT plus routine treatments compared with routine treatments in terms of alleviating pain intensity (MD,
#References 1, 4, 6, 8, 9, 12, 20, 25, 29, 31-34, 36-39, 41.
–0.97 [95% CI, –1.13 to –0.82], P < .00001, I2 ¼ 69%). A subgroup analysis was performed based on the assessment time. Compared with routine treatments, both immediate efficacy and short-term efficacy were better. The results were significant and had low heterogeneity (immediate: MD, –1.10 [95% CI, –1.27 to –0.92], P < .00001, I2 ¼ 40%; short-term: MD, –0.72 [95% CI, –0.94 to –0.50], P < .00001, I2 ¼ 39%). However, in terms of long-term efficacy,

Figure 3. Forest plot of comparison of visual analog scale (VAS) between extracorporeal shock wave therapy plus routine treatments and routine treatments. Within the figure the three time points were marked as a, b and c, and relate to before treatment, immediately after treatment and 3 months after treatment. IV, Inverse Variance.
although ESWT plus routine treatments was favored in terms of pain intensity compared with routine treatments, obvious heterogeneity was found, so reliable conclusions could not be drawn (MD, –0.90 [95% CI, –1.40 to –0.41],P < .00001, I2 ¼ 89%) (Figure 3).
Shoulder Function
Compared with routine treatments, the effectiveness of ESWT plus routine treatments on shoulder function after intervention was assessed in terms of CMS in 4 trials12,24,29,36 (SMD, 1.13 [95% CI, 0.76-1.49],
P < .00001, I2 ¼ 57%). Strong evidence was detected that ESWT plus routine treatments was more effective for improving shoulder function in terms of immediate efficacy, with no heterogeneity (SMD, 1.54 [95% CI, 1.19
1.89], P < .00001, I2 ¼ 0%) (Figure 4). However, we could not draw reliable conclusions about short- and long-term efficacy.
Joint Range of Motion
ER ROM was used to reflect the ROM, which was assessed in 4 RCTs.5,6,9,38 Because of the limited number of studies, ER ROM was measured immediately after treatment in all included studies. The pooled result of the included studies showed that the heterogeneity was high and unacceptable (MD, 10.31 [95% CI, 3.46–17.17], P < .003, I2 ¼ 93%) (Figure 5).
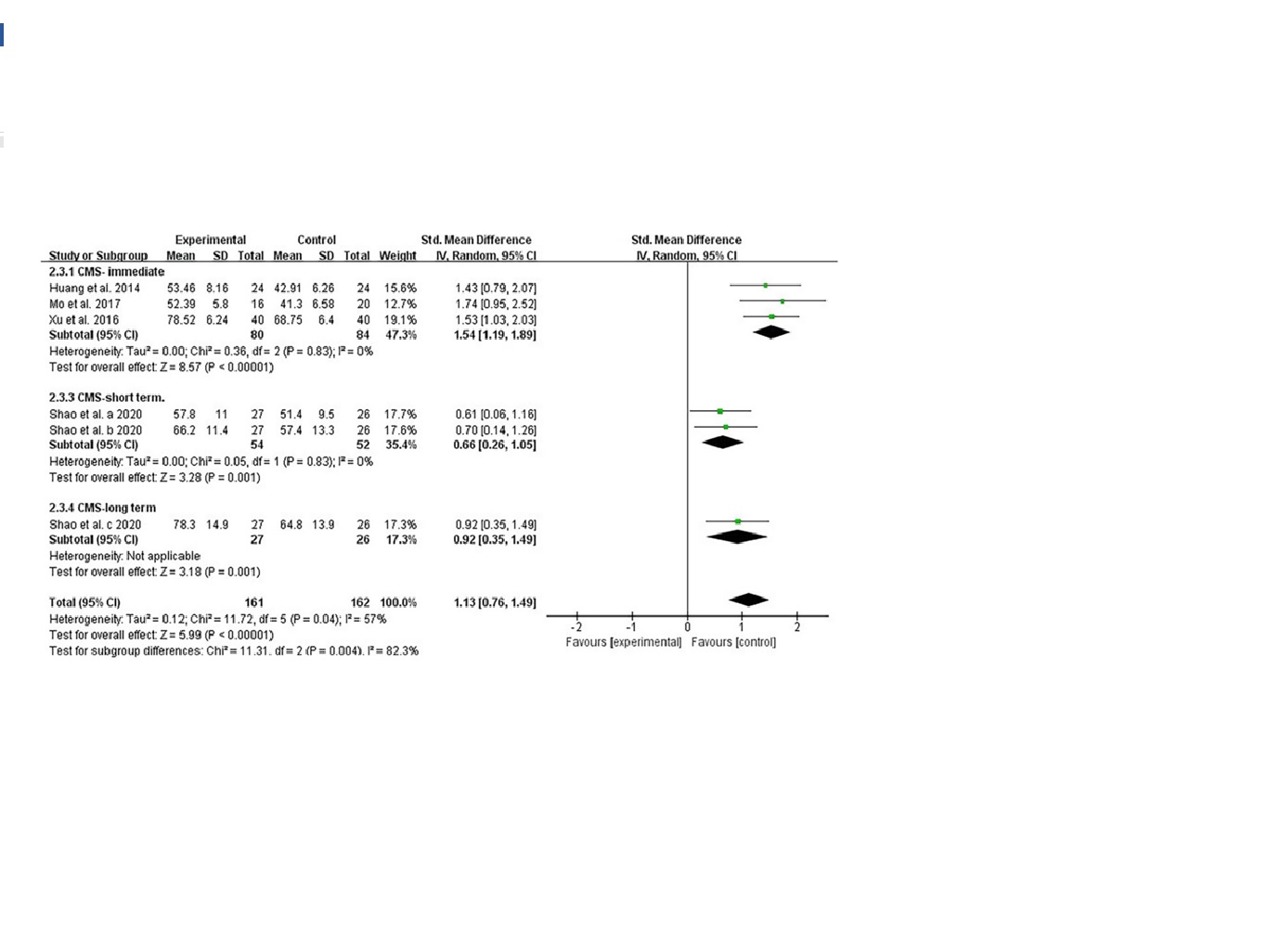
Figure 4. Forest plot of the comparison of Constant Murley score (CMS) between extracorporeal shockwave therapy plusroutine treatments and routine treatments. Within the figure the three time points were marked as a, b and c, and relate to before treatment, immediately after treatment and 3 months after treatment. IV, Inverse Variance; Std, standardized.
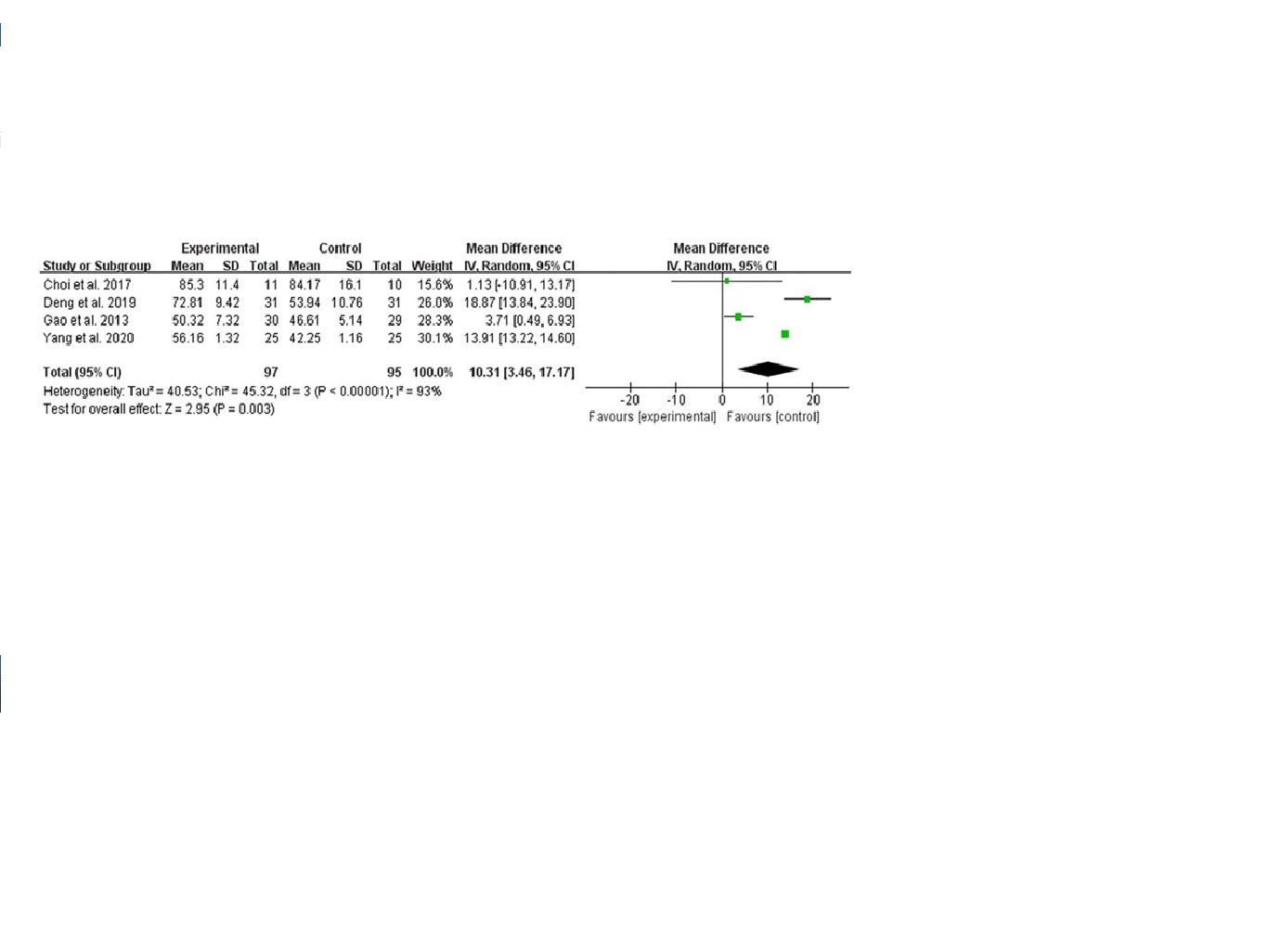
Figure 5. Forest plot of the comparison of external rotation range of movement (ER ROM) between extracorporeal shockwave therapy plus routine treatments and routine treatments. IV, Inverse Variance.
DISCUSSION
This is the first meta-analysis comparing the effectiveness of ESWT plus routine treatments and routine treatments in frozen shoulder. We preliminarily found that analgesic effects (immediate and short-term) and function (immediate) were better in the groups where ESWT was used as an adjunct to other interventions (immediate analgesic effects: MD, –1.10 [95% CI, –1.27 to –0.92], P < .00001;short-term analgesic effects: MD, –0.72 [95% CI, –0.94 to –0.50], P < .00001; immediate function: SMD, 1.54 [95% CI, 1.19 to 1.89], P < .00001, I2 ¼ 0%). However, for the improvement of long-term analgesia (MD, –0.90 [95% CI,–1.40 to –0.41], P < .00001, I2 ¼ 89%) and external rotation of the shoulder joint (MD, 10.31 [95% CI, 3.46 to 17.17],
P < .003, I2 ¼ 93%), although there was evidence pointing to the effectiveness of ESWT plus routine treatments com- pared with routine treatments, the data were heterogeneous, and the conclusions were not reliable. In addition, because of the limited number of studies and the fact that data reflecting short-term and long-term improvement in shoulder function relied on the same RCT,29 we could not prove that ESWT as an adjuvant therapy better promotes the improvement of shoulder function.
The pathophysiology of frozen shoulder remains unclear. Although disagreements exist, cytokine-mediated synovial inflammation with fibroblastic proliferation is the most recognized explanation.22 Increased expression levels of growth factors, cytokines, and matrix metal oproteinases are found in the patient’s capsular biopsy specimens,
Suggesting that these substances are involved in the inflammatory and fibrotic cascade of frozen shoulder.7
ESWT refers to a series of acoustic pulses with a certain energy density transmitted to a specific target area via an appropriate generator, thus achieving therapeutic effect.28
First, the energy emitted via shockwaves can reach the affected area via body fluid and tissue, improve the distribution of local blood flow, promote the activation of molecular and immunological reactions, stimulate angiogenesis, promote microcirculation, increase cell oxygen carrying, produce anti-inflammatory effects, and alleviate pain.10,14,15 Second, ESWT can up regulate nitric oxide levels, promote the ingrowth of endothelial nitric oxide
synthase activity, and down regulate nuclear factor kappa B expression.21 Third, shockwave therapy can produce a cavitation effect between tissues, cause intertissue release, promote the separation of adhesion, and release the adhesive tissue.23 Fourth, this method can change the acceptance frequency of nociceptors to pain, change the composition of chemical mediators around nociceptors, cause changes in free radicals around cells, release sub- stances that inhibit pain, and inhibit the transmission of pain information.10 Fifth, local high-intensity shockwaves can produce super stimulation to nerve endings, reduce nerve sensitivity, hinder nerve conduction function, and relieve pain.35 Finally, intensification of tissue regeneration, decrease in tissue apoptosis, and effective recruitment of fibroblasts have been observed in some basic studies.16
Study Limitations
There are some potential limitations that should be addressed in this study. First, because of the time overlap, the clinical stages of disease were not completely uniform. The vast majority were in the adhesive phase, and a small number were in the overlap of the painful freezing phase and adhesive phase. Second, because of the limited number of studies included, we were not able to perform further subgroup analysis on the results with high heterogeneity, or the studies included in subgroup analysis were insufficient, resulting in incomplete conclusions. Third, the characteristics of each included population were inevitably different, which more or less reduced the reliability and clinical applicability of the results to some extent. Clinical trials should be standardized in the future so that meta- analyses will better elaborate subgroups, including stages of frozen shoulder, main symptoms, comorbidity, and sex.
CONCLUSION
Although the quality level of the included RCTs was limited, based on this meta-analysis, we can conclude that ESWT seems to be beneficial to patients with frozen shoulder by alleviating pain and improving function. ESWT could be used as an adjunct therapeutic method to routine treatments. Considering methodological imperfections, future multicenter, prospective clinical trials with large sample sizes, placebo control, successful blinding, and effective follow up are needed.
REFERENCES
1.Cai ZZ, Lin SZ, Huang ZX. Application of extracorporeal shock wave combined with joint cavity and pain point block in the treatment of severe shoulder periarthritis. Article in Chinese. Contemp Med. 2019;
25(24):81-84.
- 2. Chaudhury S, Gwilym SE, Moser J, Carr AJ. Surgical options for patients with shoulder Nat Rev Rheumatol. 2010;6:217-226.
- Chen CY, Hu CC, Weng PW, et al. Extracorporeal shockwave therapy
improves short-term functional outcomes of shoulder adhesive cap- sulitis. J Shoulder Elbow Surg. 2014;23:1843-1851.
- Chen Y, Peng X, Tang ZW, Lu M. Therapeutic effects of mobilization
combined with extracorporeal shock wave treatment on patients with scapulohumeral periarthritis. Article in Chinese. Chin J Rehabil. 2014;
3:192-194.
- Choi JH, Kim SH, AnHJ, Koo JP, Kim NJ. Effects of 6 week kinesio taping and extracorporeal shock wave therapy on the joint range of
motion in patients with frozen shoulder. J Int Acad Phys Ther Res.
2017;8(1):1095-1099.
- Deng XZ, Yuan HX. Therapeutic effect of joint mobilization and ultra- short wave combined with extracorporeal shock wave on periarthritis
of shoulder. Article in Chinese. Med Inf. 2019;32(11):108-110.
- Dias R, Cutts S, Massoud S. Frozen shoulder. BMJ. 2005;331(7530):
1453-1456.
- Ding HT, Tang XZ, Jia YF, Chen J. Clinical observation of shock wave combined with massage on periarthritis of shoulder. Article in Chi-
nese. Chin J Rehabil Med. 2013;28(5):468-470.
- Gao K, Zhu XC, Yue LH, Feng J, Shen K. Extracorporeal shock wave combined with functional training for the treatment of frozen shoulder.
Article in Chinese. China J Orthop Trauma. 2013;26(5):401-403.
- Han NH, Liu MY, Chu HZ, et al. Meta-analysis of the clinical effect of extracorporeal shock wave therapy in the treatment of scapulohum-
eral periarthritis. Article in Chinese. Int J Lab Med. 2020;41(12):
1412-1417.
- Higgins JPT, Altman DG, Gøtzsche PC, et al. The Cochrane Colla- boration’s tool for assessing risk of bias in randomised trials. BMJ.
2011;343:d5928.
- 12. Huang J, Peng Y, Tang R. Clinical observation of extracorporeal shock wave combined with joint loosening in the treatment of periar-
thritis of shoulder. Article in Chinese. J Mil Surg Southwest China.
2014;16(6):635-636.
- Hussein AZ, Donatelli RA. The efficacy of radial extracorporeal shock- wave therapy in shoulder adhesive capsulitis: a prospective, rando-
mised, double-blind, placebo-controlled, clinical study. Eur J Physiother. 2016;18:63-76.
- Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension state-
ment for reporting of systematic reviews incorporating network metaanalyses of health care interventions: checklist and explana-
tions. Ann Intern Med. 2015;162:777-784.
- Jain TK, Sharma NK. The effectiveness of physiotherapeutic interven- tions in treatment of frozen shoulder/adhesive capsulitis: a systematic
review. J Back Musculoskelet Rehabil. 2014;27:247273.
- Kabbabe B, Ramkumar S, Richardson M. Cytogenetic analysis of the pathology of frozen shoulder. Int J Shoulder Surg. 2010;4:75-78.
- Kwaees TA, Charalambous CP. Surgical and non-surgical treatment
of frozen shoulder: survey on surgeons treatment preferences. Mus- cles Ligaments Tendons J. 2014;4:420-424.
- Laslett LL, Burnet SP, Jones JA, Redmond CL, McNeil JD. Musculo-
skeletal morbidity: the growing burden of shoulder pain and disability and poor quality of life in diabetic outpatients. Clin Exp Rheumatol.
2007;25:422-429.
- Le HV, Lee SJ, Nazarian A, Rodriguez EK. Adhesive capsulitis of the shoulder: review of pathophysiology and current clinical treatments.
Shoulder Elbow. 2017;9(2):75-84.
- Li SC. Clinical observation of joint loosening combined with extracor- poreal shock wave in the treatment of periarthritis of shoulder. Article
in Chinese. Gen J Stomatol. 2018;5(32):179-180.
- Mariotto S, de Prati AC, Cavalieri E, Amelio E, Marlinghaus E, Suzuki
- H. Extracorporeal shock wave therapy in inflammatory diseases:
molecular mechanism that triggers anti-inflammatory action. Curr
Med Chem. 2009;16:2366-2372.
- Mezian K, Coffey R, Chang KV. Frozen shoulder. In: StatPearls [Inter- net]. StatPearls Publishing; 2020.
- Min L, Xiao Y, Tang RL, et al. Advances in clinical research on the treatment of periarthritis of shoulder by extracorporeal shock wave. Article in Chinese. World Latest Med Inf. 2017;7(14):87-88.
- Mo XX, Zheng RX, Ouyang ZL, Wu RK. Clinical observation of warm- ing acupuncture combined with extracorporeal shock wave in treating periarthritis of shoulder. Article in Chinese. Inner Mongolia Tradit Chin Med. 2017;36(Z1):184-185.
- Qin XD, Cao XC, Fu Q, Gao CH. Effect of exogenous shock wave combined with Maitland manipulation on periarthritis of shoulder. Arti-
cle in Chinese. Chin J Phys Med Rehabil. 2013;7:571-572.
- Rangan A, Brealey SD, Keding A, et al. Management of adults with primary frozen shoulder in secondary care (UK FROST): a multicentre, pragmatic, three-arm, superiority randomised clinical trial. Lancet.
2020;396(10256):977-989.
- Rangan A, Hanchard N, McDaid C. What is the most effective treat- ment for frozen shoulder? BMJ. 2016;354:i4162.
- Reilly JM, Bluman E, Tenforde AS. Effect of shockwave treatment for management of upper and lower extremity musculoskeletal condi- tions: a narrative review. PM R. 2018;10(12):1385-1403.
- Shao JC, Sun YN, Li J, Zhu HQ, Wang SK, Li JY. The clinical efficiency and safety of extracorporeal shock wave therapy in treatment of dia- betes mellitus complicated by periarthritis of shoulder. Article in Chi- nese. Hebei Med J. 2020;42(8):1192-1195.
- Vahdatpour B, Taheri P, Zade AZ, Moradian S. Efficacy of extracor- poreal shockwave therapy in frozen shoulder. Int J Prev Med. 2014;5:
875-881.
- Wang X. Observation on therapeutic effect of acupuncture with extra- corporeal shock wave on peripheral-shoulder. Article in Chinese. World Latest Med Inf. 2018;18(76):155-156.
- Wang XC, Hao LS, Chen J. Clinical study on divergent type extra- corporeal shock wave therapy combined with intra-articular
injection and functional exercises in the treatment of periarthritis humeroscapularis. Article in Chinese. Trad Chin Orthop Trauma.
2017;29(8):36-38.
- Wu DW, Huang XB, Lyu LM, Tang SS. A clinical research on radial extracorporeal shock wave combined with intra-articular injection for treatment of frozen shoulder. Article in Chinese. Anhui Med Pharm J.
2017;21(12):2274-2277.
- Xie G, Yao HY, Wang L, Ouyang PF, Yaxi LV. Effect of joint mobili- zation combined with extracorporeal shock wave on scapulohum- eral periarthritis. Article in Chinese. Med Innov China. 2019;16(26):
28-31.
- Xing GY, Zhang PG, Shi Z, et al. Extracorporeal shock wave therapy combined with arthroscopy for the treatment of osteochondral lesions
of the talus. Orthop J China. 2011;19(12):978-981.
- Xu L, Li XP, Gao MX. Effect of extracorporeal shock wave and manip- ulation treatment in scapulohumeral periarthritis. Article in Chinese. J Clin Exp Med. 2016;15(16):1574-1577.
- Yang J, Liao ZB, Zhou RJ, Zhou GH. Effect of extracorporeal shock wave on pain of periarthritis of shoulder. Article in Chinese. Chin Foreign Med Res. 2017;2:22-23.
- 38. Yang QX, Tan YS. Treatment of scapulohumeral periarthritis with massage combined with extracorporeal shock wave. Article in Chin Manip Rehabil Med. 2020;7:36-38.
- Yang Y, Huang GC, Dong M. Observation on extracorporeal shock wave therapy and traditional Chinese medicine fumigation in the treatment of frozen shoulder. Article in Chinese. Mod Med Health.
2019;35(14):2123-2125.
- Zhang J, Zhong S, Tan T, et al. Comparative efficacy and patient- specific moderating factors of nonsurgical treatment strategies for frozen shoulder: an updated systematic review and network meta-
analysis. Am J Sports Med. 2021;49(6):1669-1679.
- Zhang TH, Yan RX, Sun TS, Tian YD, Zhou SH. Clinical observation of pain point injection combined with shock wave in treating periarthritis of shoulder. Article in Chinese. Chin J Ctrl Endem Dis. 2016;31(11):
1248-1249.
APPENDIX
TABLEA1
Details of the PubMed Search Strategy
#1 Search “Frozen shoulder”[MeSH]
#2 Search: (((((((((((((((((((((frozen shoulder[Title/Abstract]) OR (Bursitides[Title/Abstract])) OR (Bursitis[Title/Abstract])) OR (Frozen Shoulders[Title/Abstract])) OR (Shoulder, Frozen[Title/Abstract])) OR (Adhesive Capsulitis of the Shoulder[Title/Abstract])) OR (Shoulder Adhesive Capsulitis[Title/Abstract])) OR (Adhesive Capsulitides, Shoulder[Title/Abstract])) OR (Adhesive Capsulitis, Shoulder[Title/Abstract])) OR (Capsulitides, Shoulder Adhesive[Title/Abstract])) OR (Capsulitis, Shoulder Adhesive[Title/ Abstract])) OR (Shoulder Adhesive Capsulitides[Title/Abstract])) OR (Capsulitis[Title/Abstract])) OR (Capsulitides[Title/ Abstract])) OR (Pes Anserine Bursitis[Title/Abstract])) OR (Bursitides, Pes Anserine[Title/Abstract])) OR (Bursitis, Pes Anserine[Title/Abstract])) OR (Pes Anserine Bursitides[Title/Abstract])) OR (Adhesive Capsulitis[Title/Abstract])) OR (Adhesive Capsulitides[Title/Abstract])) OR (Capsulitides, Adhesive[Title/Abstract])) OR (Capsulitis, Adhesive[Title/Abstract])
#3 Search “Extracorporeal Shockwave Therapy”[MeSH]
#4 Search: ((((((((((((((Extracorporeal Shockwave Therapies[Title/Abstract]) OR (Shockwave Therapies, Extracorporeal[Title/Abstract])) OR (Shockwave Therapy, Extracorporeal[Title/Abstract])) OR (Therapy, Extracorporeal Shockwave[Title/Abstract])) OR (Shock Wave Therapy[Title/Abstract])) OR (Shock Wave Therapies[Title/Abstract])) OR (Therapy, Shock Wave[Title/Abstract])) OR (Extracorporeal Shock Wave Therapy[Title/Abstract])) OR (Extracorporeal High-Intensity Focused Ultrasound Therapy[Title/ Abstract])) OR (Extracorporeal High Intensity Focused Ultrasound Therapy[Title/Abstract])) OR (HIFU Therapy[Title/Abstract])) OR (HIFU Therapies[Title/Abstract])) OR (Therapy, HIFU[Title/Abstract])) OR (High-Intensity Focused Ultrasound Therapy[Title/Abstract])) OR (High Intensity Focused Ultrasound Therapy[Title/Abstract])
#5 Search (randomized controlled trial[Publication Type]OR randomized[Title/Abstract] OR placebo[Title/Abstract])
#6 #1 OR #2
#7 #3 OR #4
#8 #5 AND #6 AND #7
TABLEA2
Basic Features of the Included Studiesa
|
|
Sample |
|
|||||
|
Size |
|||||||
|
Lead Author |
(ESWT/ |
|
|
Intervention |
|
Measurement |
|
|
(Year) |
Control) |
ESWT Group |
Control Group |
Time |
Follow-up |
Time |
Outcomes |
Cai (2019)1 40/40 ESWT þ pain point injection þ intra-articular injectionb þ manual therapy
Pain point injection þ intra-articular injectionb þ
manual therapy
2 wk 3 mo Before treatment and 3 mo after treatment
VAS
Chen (2014)4 35/35 ESWT (1500 shockwaves, 10 Hz,
1.5 bar) þ manual therapy
Choi (2017)5 11/10 ESWT (800 impulses, 5 Hz,
0.129 mJ/mm2) þ kinesio taping
Manual therapy Once every 6 d for
20 d
Kinesio taping Twice a wk for
4 wk
NR Before and after treatment
NR Before and after treatment
VAS
ER ROM
Deng (2019)6 31/31 ESWT (2000 waves, 8 Hz,
1.0 bar) þ ultra-short-wave therapy þ joint loosening
Ultra-short-wave therapy þ joint loosening
Once every 6 d for
30 d
NR Before and after treatment
VAS, ER ROM
Ding (2013)8 65/63 ESWT (2000 shockwaves,
4.5 J) þ massage
Massage 3 /wk (10 total) NR Before and after treatment
VAS
Gao (2013)9 30/29 ESWT (600-2000 shocks,
12-15 Hz, 1.6-2.5 bar) þ
routine rehabilitation therapy
Routine rehabilitation therapy
Once a wk for
3 wk
NR Before and after treatment
VAS, ER ROM
Huang
(2014)12
24/24 ESWT (1000 impulses,
0.18-0.25 mJ/mm2) þ routine rehabilitation therapy
Routine rehabilitation therapy
Once a wk for
3 wk
NR Before and after treatment
VAS, CMS
Li (2018)20 42/42 ESWT (1500 shockwaves, 10 Hz,
5 bar) þ manual therapy
Manual therapy Once every 6 d
(2 total)
NR Before and after
Treatment
VAS
Mo (2017)24 16/20 ESWT (2500-3500 waves,
10-15 Hz, 1.5-2.8 bar) þ
Warming
Qin (2013)25 23/23 ESWT (1500-2000 shocks, 6.5-11.0 kV) þ routine rehabilitation therapy
Warming acupuncture
Routine rehabilitation therapy
Once every 5 d for
25 d
Once every -7 d for 1mo
NR Before and after treatment
NR Before and after treatment
CMS VAS
Shao
(2020)29
Wang
(2017)32
Wang
(2018)31
27/26 ESWT (1200 shocks,0.25mJ/mm2) þ oral corticosteroid þ transcutaneous electrical nerve stimulation
63/63 ESWT (2000 waves,0.16 mJ/mm2) þ intra- articular injectionc þ manual therapy
|
Acupuncture
Oral corticosteroid þ transcutaneous electrical nerve stimulation
Intra-articular injectionc þ manual therapy
Once a wk for
6 wk
Once every 2 wk for 8 wk
NR Before treatment and 2, 6, and
12 wk after
treatment
NR Before and after treatment
VAS, CMS
VAS
Wu (2017)33 53/53 ESWT (2000 shocks,0.16-2 mJ/mm2) þ intra- articular injection
Intra-articular injection
Once a wk for
3 wk
6 wk Before treatment and 6 wk after treatment
VAS
Xie (2019)34 43/44 ESWT (2000 shockwaves,
8 Hz) þ manual therapy
Xu (2016)36 40/40 ESWT (1000 shockwaves, 10 Hz,
0.18-0.25 mJ/mm2) þ manual therapy
Manual therapy Once every 5 d for
20 d
Manual therapy Once a wk (20 d total)
NR Before and after treatment
NR Before and after treatment
VAS
VAS, CMS
Yang
(2017)37
26/26 ESWT (1000-1500 shocks,
50-60 Hz) þ routine rehabilitation therapy
Routine rehabilitation therapy
Once every 5 d
(3 total)
NR Before and after treatment
VAS