 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Tesla
Tesla Nikola
Nikola Kayser
Kayser Fusion
FusionA randomized controlled trial of ultrasound-guided pulsed radiofrequency for patients with frozen shoulder
- Type: Free
1. Introduction
Frozen shoulder (FS) is one of the most common disorders of the joint diseases.[1–3] It mainly manifests with shoulder pain and motion limitation.[4–6] It has been reported that this condition can affect 2% to 5% of the general population, mostly among the female population between 40 and 65 years old.[7–11] A variety of studies tried to explore its mechanism.[12–14] Unfortunately, it is still unclear.[11]
Several approaches have been reported to manage this condition. These managements consist of medication, physical therapy and exercise, location injections, manipulation under anesthesia, arthroscopic capsular release, muscle release, ultra- sound therapy, massage, laser therapy, and acupuncture.[15–25] However, their efficacy is still limited.
Although ultrasound-guided pulsed radiofrequency (UGPRF) has also been reported to treat FS,[26] there is still insufficient data to support this therapy. The lacking evidence for UGPRF for the treatment of FS warrants strictly designed randomized clinical trials (RCTs). Therefore, in this RCT study, we hypothesized that for treatment of FS, the effectiveness of UGPRF would be superior to the effectiveness of sham UGPRF.
2. Methods and design
- Ethical approval
The present study was approved by the ethics committee of Yanan University Affiliated Hospital, and The First People’s Hospital of Xianyang City. All included patients were asked to provide the written informed consent before the study.
- Study design
This study was designed as a randomized, double-blind, sham- control trial with 2 parallel groups. A total of 136 eligible patients with FS were recruited from Yanan University Affiliated Hospital and The First People’s Hospital of Xianyang City by poster or advertise from January 2017 to June 2018. After screening, all included subjects were randomly allocated to a treatment group or a control group in a ratio of 1:1. Before the randomization, there was be a 1 week run-in period. Patients in both groups were
treated for a total of 12 weeks. All outcomes were assessed at baseline, at the end of 6 weeks and 12 weeks treatment.
- Patients
The inclusion criteria included patients aged between 40 and 70 years with 1 side shoulder attacked; primary idiopathic adhesive capsulitis; experiencing shoulder pain and motion limitation at least 3 months before the study.
Patients were excluded if they did not agree to participate or continue the study; having systematic diseases, bony abnormali- ty, calcific tendonitis, shoulder osteoarthritis, psychological disorder, photoallergy, substantial local trauma history, previous shoulder surgery, local infection, relex sympathetic dystrophy, pregnancy, or breastfeeding; receiving UGPRF, or physiotherapy treatment during the last 3 months before the study; or using anti- pain medication during this study.
- Randomization and blinding
A random number list was generated through SAS 9.1 package (SAS Institute Inc., Cary, NC) by a specified research assistant who was masked to the study allocation. Stratified randomiza- tion was performed to randomize and allocate the patients equally to a treatment group and a sham group in a 1:1 ratio by using concealed in sequentially numbered, opaque, sealed envelopes. Attending investigators, subjects, outcome assessors, as well as the data analysts were blinded in this study.
- Intervention
The patients in the treatment group received UGPRF. Under sterile conditions and appropriate monitoring, the subjects were placed in a seated position on a chair. Local skin and soft tissues were anesthetized with 1 mL 2% lidocaine before the needles of radiofrequency inserted. After that, its needles and probes arrived at each target nerves under the guidance by ultrasound. Radiofrequency therapy was applied by using a 10 cm 22-gauge cannula with a 10 mm active. The sensorial stimulation was utilized to check and identify the nerve position with a threshold current intensity of <0.5 mA. The needles of radiofrequency were regarded to be adequately placed by ultrasound guidance; the current intensity was decreased to less than 0.2 mA. Then pulsed radiofrequency therapy was applied by using 2 Hz current at 40 volts with 20 ms active and 480 ms silent periods. The temperature was controlled to less than 42°C.
The patients in the sham group undergo the same procedure. The radiofrequency treatment was simulated without applying pulsed stimulation. Patients in both groups received once weekly for a total of 12 weeks intervention.
- Outcome measurements
The primary outcome of pain intensity was measured by the visual analog scale (VAS).[27] The score ranges from 0, no pain, to 10, worst. The secondary outcomes included shoulder disorder, as measured by the score of shoulder pain and disability index (SPADI), varying from 0 to 100, with score of 0 indicating less shoulder disability and 100 indicating more shoulder dysfunc- tion;[28] and quality of life, as assessed by the Short Form-36 questionnaire (SF-36), each item is scored on a 0 to 100 range, with a higher score indicating better quality of life.[29] All primary and secondary outcomes were measured at baseline, at the end of 6 weeks and 12 weeks treatment.
- Safety evaluation
Any adverse events (AEs) were monitored, recorded, and reported by investigators at each visit. All expected and unexpected AEs were monitored. For any AEs, we documented its date of onset and cease, intensity, and also the association to the intervention. Based on those reports, the physicians decided to continue treating the subjects or not.
- Data management
All data values were collected by a case report form (CRF), which specifically pre-designed by the researchers according to the standard operating procedures of the Yanan University Affiliated Hospital, and The First People’s Hospital of Xianyang City. All the data were entered into electronic database of the research computer system. Any paper records were kept in locked cabinets.
- Quality control
Two monitors from the Ethic Committee of Yanan University Affiliated Hospital and The First People’s Hospital of Xianyang City monitored all the procedures of the study, including written informed consent, protocol compliance, data collection, CRF, and all other documents filling, as well as the other study-related procedures.
- Statistical analysis
All data were analyzed by SAS 9.1 package using intent-to-treat analysis. The t test or Mann–Whitney U test was utilized to perform the continuous variables. Fisher exact test or x2 test was applied to analyze the categorical variables. A value of P <.05 was considered statistically significant.
- Sample size
To detect difference between the treatment group and the control group of at least 30% in pain intensity, measured by VAS scale, and with a=0.05, power of 80%, effect value of 0.75, the desired sample size for this RCT is 136 patients, with 68 subjects in each group, including the assumed dropout rates of 15%.[30] It is the minimum required sample size to evaluate the effectiveness UGPRF for patients with FS.
3. Results
A total of 169 potential eligible patients initially entered this study for screen (Fig. 1). After selection, 33 subjects were excluded. Thus, 136 patients were included and were divided equally into the treatment group and sham group in this study. After 6 weeks treatment, no patient in either group withdrew from the study. However, after 12 weeks treatment, 1 subject in the control group withdrew from the study, because he moved to the other city and quitted the treatment.
Baseline characteristics are summarized in Table 1. At baseline, no significant differences in all characteristics values were found between 2 groups. These values included basic characteristics, demographics, and primary and secondary outcome measure- ment at baseline.
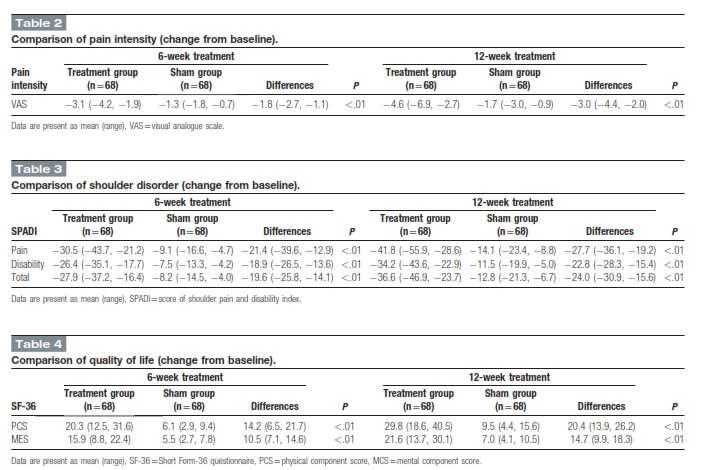
At the end of 6 weeks, and 12 weeks, patients in the treatment group exerted better efficacy in pain relief, as measured by VAS (P <.01, Table 2), improvement of shoulder disorder, as assessed by SPADI score (pain, P <.01; disability, P <.01; total, P <.01;
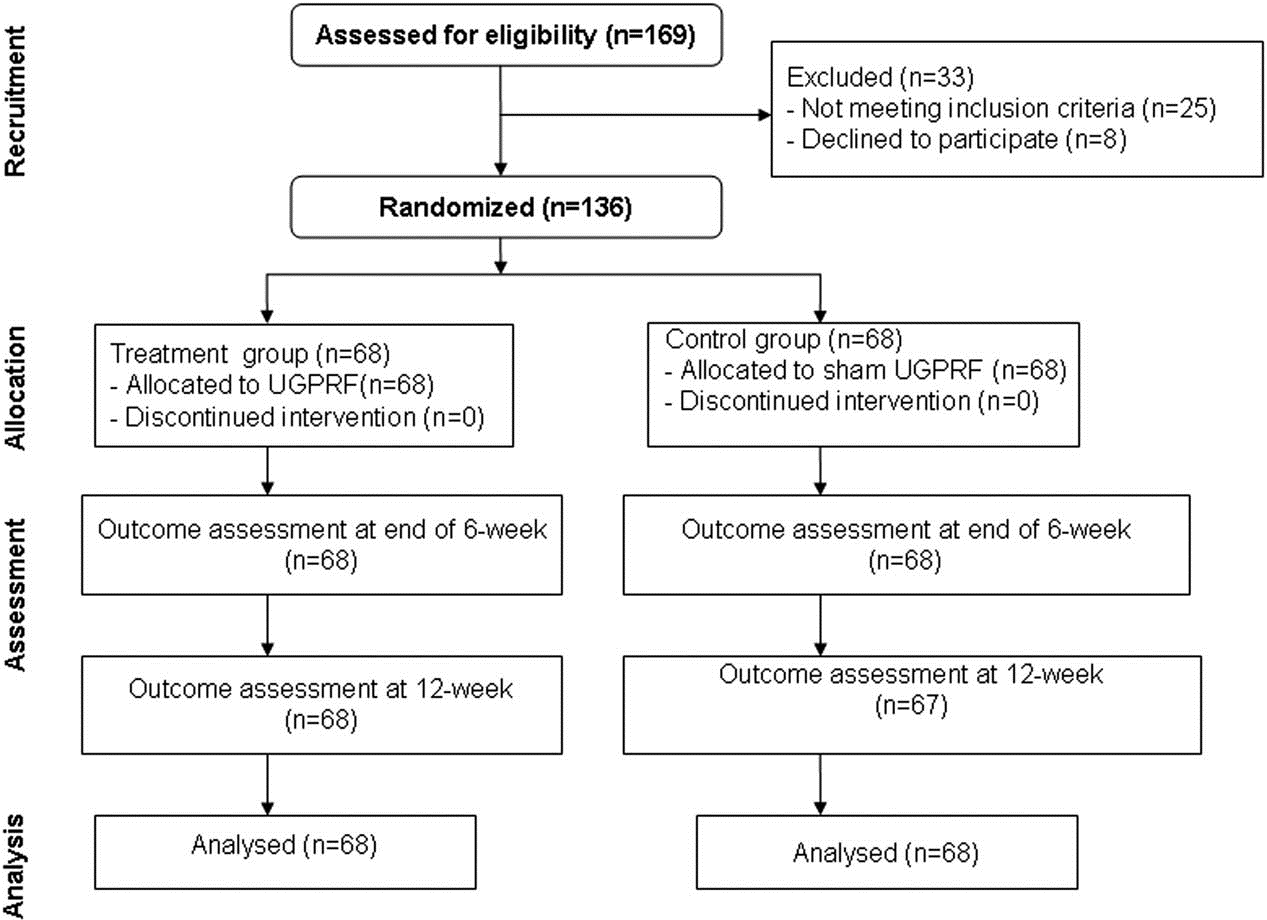
Figure 1. Flowchart of participant selection.
Table 3), and enhancement of quality of life, as measured by the SF-36 scale (PCS, P <.01; MCS, P <.01; Table 4), compared with patients in the sham group in this study.
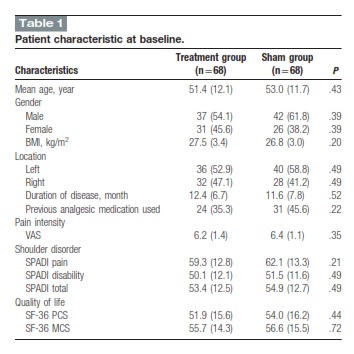
Data are present as mean ±standard deviation or number (%); BMI =body mass index, VAS = visual analogue scale, SPADI =score of shoulder pain and disability index, SF-36 = Short Form-36 questionnaire, PCS = physical component score, MCS= mental component score.
No severe AEs were recorded in either group in this study. No death related treatment occurred in both groups. However, 2 subjects reported slight pain in the treatment. Fortunately, no patients withdrew from the study because of the AEs.
1. Discussion
This randomized, double-blind, sham-control trial was designed to compare the effectiveness of UGPRF treatment with that of sham UGPRF intervention for patients suffering from FS. Reductions in pain intensity of attacked shoulders and improve- ment in shoulder mobility and quality of life were assessed to confirm whether the patients with FS were improved or not.
for the treatment of FS. To our best knowledge, this study first focused on this issue. The results of this RCT may provide very valuable evidence for the potential treatment of FS. We wish to provide a scientific basis for this management according to the results of this study. However, more stringent data are still but also can improve the status of shoulder disorder, as evaluated by SPADI score, as well as can enhance the quality of life, as measured by SF-36 scale. Moreover, only minor AEs of slight
pain were recorded in this study. It results indicated that UGPRF may be utilized as an alternative intervention for FS treatment. This study had 2 limitations. First, this study did not include follow-up assessment after the treatment quit. Thus, further studies should extend the outcome evaluation period with follow- up visit after the treatment. Second, since this study is the first study to explore the effectiveness of UGPRF for FS, therefore, more studies should be focused on this issue to further warrant the results of this study.
1. Conclusion
The results of this study demonstrated that UGPRF is more effective for patients with FS than sham UGPRF after 12 weeks treatment.
Author contributions
Conceptualization: Juan Yan, Xian-Min Zhang.
Data curation: Juan Yan, Xian-Min Zhang.
Formal analysis: Juan Yan. Investigation: Xian-Min Zhang. Methodology: Juan Yan.
Project administration: Xian-Min Zhang. Resources: Juan Yan, Xian-Min Zhang. Software: Juan Yan.
Supervision: Xian-Min Zhang.
Validation: Juan Yan, Xian-Min Zhang.
Visualization: Juan Yan, Xian-Min Zhang.
Writing – original draft: Juan Yan, Xian-Min Zhang.
Writing – review & editing: Juan Yan, Xian-Min Zhang.
References
-
Cui J, Lu W, He Y, et Molecular biology of frozen shoulder-induced limitation of shoulder joint movements. J Res Med Sci 2017;22:61.
-
Guyver PM, Bruce DJ, Rees JL. Frozen shoulder-a stiff problem that requires a flexible Maturitas 2014;78:11–6.
-
Robinson CM, Seah KT, Chee YH, et al. Frozen shoulder. J Bone Joint Surg Br 2012;94:1–
-
Kelley MJ, McClure PW, Leggin BG. Frozen shoulder: evidence and a proposed model guiding rehabilitation. J Orthop Sports Phys Ther 2009;39:135–
-
Dias R, Cutts S, Massoud S. Frozen shoulder. BMJ 2005;331: 1453–
-
Noël E, Thomas T, Schaeverbeke T, et Frozen shoulder. Joint Bone Spine 2000;67:393–400.
-
Cadogan A, Mohammed KD. Shoulder pain in primary care: frozen J Prim Health Care 2016;8:44–51.
-
Yoon JP, Chung SW, Kim JE, et al. Intra-articular injection, subacromial injection, and hydrodilatation for primary frozen shoulder: a randomized clinical trial. J Shoulder Elbow Surg 2016;25:376–
-
Bunker TD. Frozen shoulder: unravelling the enigma. Ann R Coll Surg Engl 1997;79:210–
-
Hannafin JA, Chiaia TA. Adhesive capsulitis. A treatment approach. Clin Orthop Relat Res 2000;372:95–
-
Lewis J. Frozen shoulder contracture syndrome—aetiology, diagnosis and management. Man Ther 2015;20:2–
-
Bunker TD, Reilly J, Baird KS, et al. Expression of growth factors, cytokines and matrix metalloproteinases in frozen shoulder. J Bone Jt Surg Br 2000;82:768–
-
Uhthoff HK, Boileau P. Primary frozen shoulder: global capsular stiffness versus localized contracture. Clin Orthop Relat Res 2007;456:79–
-
Tamai K, Akutsu M, Yano Primary frozen shoulder: brief review of pathology and imaging abnormalities. J Orthop Sci 2014;19:1–5.
-
Gallacher S, Beazley JC, Evans J, et al. A randomized controlled trial of arthroscopic capsular release versus hydrodilatation in the treatment of primary frozen shoulder. J Shoulder Elbow Surg 2018;27:1401–
- Shih YF, Liao PW, Lee CS. The immediate effect of muscle release intervention on muscle activity and shoulder kinematics in patients with frozen shoulder: a cross-sectional, exploratory study. BMC Muscu- loskelet Disord 2017;18:499.
- Ebadi S, Forogh B, Fallah E, et al. Does ultrasound therapy add to the effects of exercise and mobilization in frozen shoulder? A pilot randomized double-blind clinical trial. J Bodyw Mov Ther 2017;21:781–
- Kraal T, The B, Boer R, et al. Manipulation under anesthesia versus physiotherapy treatment in stage two of a frozen shoulder: a study protocol for a randomized controlled trial. BMC Musculoskelet Disord 2017;18:412.
- Chen HC, Chuang TY, Lin PC, et al. Effects of messages delivered by mobile phone on increasing compliance with shoulder exercises among patients with a frozen J Nurs Scholarsh 2017;49:429–37.
- Robinson PM, Norris J, Roberts CP. Randomized controlled trial of supervised physiotherapy versus a home exercise program after hydro- dilatation for the management of primary frozen shoulder. J Shoulder Elbow Surg 2017;26:757–
- Pushpasekaran N, Kumar N, Chopra RK, et al. Thawing frozen shoulder by steroid injection. J Orthop Surg (Hong Kong) 2017;25:
- Cho CH, Kim du H, Bae KC, et al. Proper site of corticosteroid injection for the treatment of idiopathic frozen shoulder: Results from a randomized Joint Bone Spine 2016;83:324–9.
- Kim SH, Kim YH, Lee HR, et Short-term effects of high-intensity laser therapy on frozen shoulder: a prospective randomized control study. Man Ther 2015;20:751–7.
- Celik Comparison of the outcomes of two different exercise programs on frozen shoulder. Acta Orthop Traumatol Turc 2010;44:285–92.
- Cheing GL, So EM, Chao CY. Effectiveness of electroacupuncture and interferential eloctrotherapy in the management of frozen J Rehabil Med 2008;40:166–70.
- Huang CC, Tsao SL, Cheng CY, et al. Treating frozen shoulder with ultrasound-guided pulsed mode radiofrequency lesioning of the supra- scapular nerve: two cases. Pain Med 2010;11:1837–
- Boonstra AM, Schiphorst Preuper HR, Balk GA, et Cut-off points for mild, moderate, and severe pain on the visual analogue scale for pain in patients with chronic musculoskeletal pain. Pain 2014;155: 2545–50.
- Heald SL, Riddle DL, Lamb RL. The shoulder pain and disability index: the construct validity and responsiveness of a region-specific disability Phys Ther 1997;77:1079–89.
- Lyons RA, Perry HM, Littlepage BN. Evidence for the validity of the short-form 36 questionnaire (SF-36) in an elderly population. Age Ageing 1994;23:182–
- Dworkin RH, Turk DC, McDermott MP, et Interpreting the clinical importance of group differences in chronic pain clinical trials: IMMPACT recommendations. Pain 2009;146:238–44.





