 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Tesla
Tesla Nikola
Nikola Kayser
Kayser Fusion
Fusioneffects of 6 Week Kinesiotaping and Extracorporeal Shock Wave Therapy on the Joint Range of Motion in Patients with Frozen Shoulder
- Type: Free
This study used both kinesiotaping and extracorporeal shock wave therapy on patients diagnosed with frozen shoulder - a common musculoskeletal disorder in adults - in order to observe the effects on the joint range of motion. 21 adult(male 12, female 9) were selected and distributed into randomized groups. One group received kinesiotaping (n=10) and the other group received kinesiotaping together with extra- corporeal shock wave therapy (n=11). After a 6 week duration of receiving kinesiotaping and extracorporeal shock wave therapy, changes in the joint range of motion in the patients were observed. Post-treatment of frozen shoulder, the changes in abduction within the shoulder joint were as follows: in both groups there was a noticeable increase in the joint range of motion (p<.05). Post-treatment of frozen shoulder, the changes in external rotation within the shoulder joint were as follows: both groups showed a significant increase in the joint range of motion (p<.05). The result of suggest that, it can be inferred that both the extracorporeal shock wave therapy and kinesiotaping are effective in increasing the joint range of motion in patients with frozen shoulder.
INTRODUCTION
Frozen shoulder is a common disorder that occurs in the shoulder joint of adults where the surrounding tissue suffers from degeneration as we l as various other causes, leading to joint capsule reduction, volume decrease in the joint cavity, and histologically fiber hyperplasia 1). Furthermore, thickening of the synovial membrane causes adhesion to the joint surface, leading to a steady increase in pain and a gradual decrease in the joint range of motion. While the disorder itself does not cause abrasions to the cervical nerve root or nerve related muscular weakness, the limitations placed on the joint range of motion due to pain as we l as the di ficulty experienced a tempting day to day motions is a very apparent reality 2).
Extracorporeal shock wave therapy (ESWT) is utilized in treating musculoskeletal disorders, and while the exact mechanisms behind the treatment
have yet to be discovered, its continued use receives support from two theories. The first the- ory suggests that the repeated application of ESWT on the affected area causes temporary microdamage, prompting growth of new blood vessels and increasing the blood flow to the dam- aged tissue accelerating the healing process 3). The second theory is one that stems from the dulling of the ability of the central nervous system to rec- ognize chronic pain. When chronic pain occurs in the body, the brain adapts to the pain, leading to a slowed healing reaction. As a counteraction, the ESWT causes micro damage to the area and re activates the healing reaction in the area 4).
Amongst kinesiotaping, elastic taping is applied to normalize the movement of the main muscle of the acting joint 5). Kinesiotape was developed by Dr. Kase Kenzo with the understanding that the muscle was the cause of disorders, leading to the development of tape with elasticity in accordance
J.H. Choi, S.H. Kim, H.J. H.J. An, et al.
with his belief that an elastic tape contracting with the muscle would be more effectual than tape that stays fixed on the body 6). Kinesio tape has multiple uses in the clinical setting as it aids in maintenance of postural stability, increase in proprioception, as well as circulation within lymph, blood, and tissue 7,8). Previous study reported that taping assists in creating normal shoulder joint motion by restricting the hyper mobilized muscle around the shoulder and fixating against scapular displacement as well as correcting and securing the action of the muscles surrounding the scapula 9). Research from Ackemann et al. reported that taping methods could aid in providing continuous proprioceptive sensory feedback as well as maintaining scapular disposition 10).
As evidenced, ESWT and kinesiotaping are both effective treatment methods in musculoskeletal disorders. However, there is a lack of research studying the effects of both approaches used in conjunction. As such, this study uses both kinesiotaping and ESWT on adults diagnosed with frozen shoulder in order to observe the effects on the joint range of motion, and in turn become a point of reference for alternative treatment methods of frozen shoulder as a primary source.
METHODS
21 subjects diagnosed with frozen shoulder from “H”hospital in Cheon an were chosen between February 2016 and July 2016. Subjects with frozen shoulder that showed no abnormalities on hematological tests, no other anatomical deformity other than degeneration of the joint on the basic x-ray examinations of the shoulder joint, and no anomaly
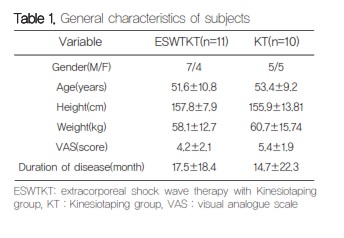
during the infrared thermography were chosen. The purpose and methods of the study were explained to the participants and an informed consent was obtained from each individual in accordance with the principles of the Helsinki Declaration.
Subjects were divided at random into two groups. One group received application of kinesiotaping (n=10) and the other group received both kinesio- taping and ESWT together (n=11).
On the first day of the study, all subjects had the joint range of motion of their shoulder joint measured with a goniometer. To keep homogeneity between the subjects, a visual analogue scale (VAS) was used. After 4 weeks, the joint range of motion of the subjects was measured again to observe the changes.
Apply of ESWT
The ESWT used was an Intelect RPW unit 2074 (KOASTRON, USA). In was applied twice a week for a duration of 4 weeks. The ESWT was applied on the area of the shoulder where the patient would complain most of pain. The energy intensity of the ESWT was placed at 800 impulses, 5Hz, and
0.129 mJ/mm 2,11).
Apply of Kinesiotape
The application of tape was done by a physio- therapist with 10 years of clinical experience using taping as a treatment method. As it was foreseen that the effects of the tape would decrease along with the adhesion of the tape to the skin, the sub- jects were told to wear the taping for a duration of 12-24 hours. The taping method used are as fol- lows5). The therapist should attach one side of the tape to the most opposite side of the most promi- nent vertebra at the junction of the cervical and thoracic spine. While the subject looks away from the affected shoulder, the physiotherapist should pull the tape with considerable stretch diagonally downward and outward across the inside upper corner of the shoulder blade to behind the outer corner past, not over, this corner continuing in a slight arc downward to the front of the upper arm of the subject. The second tape should then be applied on the lower corner of the shoulder blade with the long end of the tape pointing diagonally up toward the shoulder. The tape should then be pulled in this direction past the front outer corner of the subject’s shoulder to the back of the upper arm.
Data Analysis
The SPSS ver. 19.0 was used for the ordinary and special frequency analysis of each group. In order to find the changes of the pre and post treatment joint range of motion within each group, the paired t-test was used. The independent t-test was used to find the differences between the group.The significance level of this study was set at ɑ .05.
RESULTS
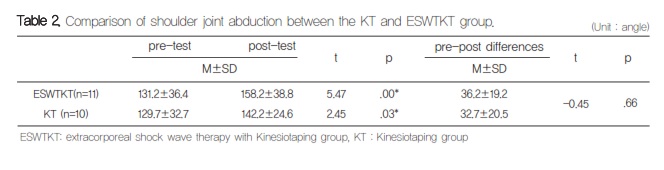
Comparison of shoulder joint abduction between the KT and ESWTKT group
The change in abduction of the shoulder joint post-treatment are as follows. Both the KT and ESWTKT groups showed a significant increase in joint range of motion (p<.05). However, there appeared to be no differences between the two groups.
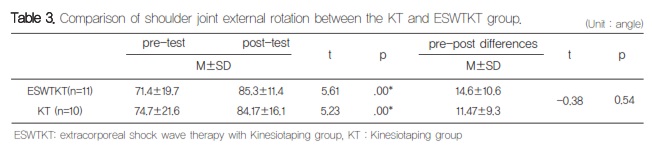
Comparison of shoulder joint external rotation between the KT and ESWTKT group
The change in external rotation of the shoulder joint post-treatment are as follows. Both the KT
and ESWTKT groups showed a significant increase in the joint range of motion (p<.05). However, there appeared to be no differences between the two groups.
The cause of frozen shoulder may divided in internal and external factors, however in most cases, the regression of the rotator cuff and long head of the biceps tendon are the leading cause. For most patients, conservative treatment alone is enough for a full recovery. For the few which this is not the case, chronic pain and limitation of motion become an inevitable handicap for many years 12). As such, this study applies both kinesio- taping and ESWT on adults suffering from this common musculoskeletal disorder frozen shoulder in order to observe the effects on the joint range of motion.
Post-treatment, both treatment groups experi- enced a significant increase in the joint range of motion in abduction and external rotation.
The following research suggest positive effects of ESWT as a treatment method for pain and functional repair in musculoskeletal disorders. In a study by Pattrone and McCall, 108 patients with chronic lateral epicondylitis were treated using ESWT and observation of the changes in pain showed that 61% of patients experienced pain reduction 13). SImilarly, Lee et al. conducted a study on patients with myofascial pain syndrome in the upper trapezius by ESWT treatment for a duration of 4 weeks and reported results that showed not only a reduction in pain but also an
increase in the joint range of motion in the shoulder joint14). In this study, while the ESWTKT group also experienced an increase in range of motion, the results cannot attribute the change to the e fects of the ESWT treatment alone. However, the causation of micro damage resulting in creation of blood vessels and stimulation of healing may be considered likely in the reduction of pain 3,4).
Tantawy and Kamel conducted a study in which 74 women who had undergone modified radical mastectomy were divided into a group which underwent conventional physiotherapy and another group that received kinesiotaping in addition to the conventional physiotherapy 15). The results showed that the latter group had a statistically significant decrease in shoulder pain and increase in joint range of motion. Gӧksu et al. pursued a study on 61 patients with subacromial impingement syndrome dividing the subjects into two groups: one group receiving kinesio taping and the other receiving local injection therapy 16). The study was conducted over a period of 4 weeks
- 3 session per week and it was reported that pain reduction and increase in joint range of motion was observed in both groups. Similarly, both groups in this study showed that application of kinesiotaping resulted in an increase in joint range of motion. The reason may be attributed to the stimulation caused by the adhesive nature or vibration, temperature difference etc. which excites the gamma motor neuron and leads to the integumentary muscle contracting also referred to as cutaneous fusimotor reflex 17,18). As such, the continuous kinesiotaping applied around the shoulder joint may have induced muscle contractions and stimulated the cerebellum as well as the reticular formation of the brain stem. As a result, the balance of the muscle tension and bodily adjustment would be influenced reforming the joint range of motion
This study lacks a large pool of participating subjects limiting the the capacity for generalization. Application of the ESWT was also dependant on the subjective input of the subject and there- fore make an exact measurement of the effect difficult. Lastly, difficulty in restricting the mobility of the subjects made regulation of the time duration in which the kinesio tape was applied unequal.
CONCLUSIONS
In this study, significant increase in abduction and external rotation of the shoulder joint was observed from both the group where kinesiotaping alone was applied and the group where kinesio- taping and ESWT were applied in conjunction. As such, it can be inferred that kinesiotaping and ESWT as a treatment for patients with frozen shoulder, aids in the increase of joint range of motion. However, changes to the duration of kinesiotape application and the electrical variables as well as per week apply of the ESWT could have a varied influence on patients with frozen shoulder. Therefore it is recommended that this area needs further continued study.
REFERENCES
- Miyazaki AN, Santos PD, Silva LA, Sella GD, Carrenho L, Checchia Clinical evaluation of arthroscopic treatment of shoulder adhesive capsulitis. Rev Bras Ortop. 2016; 52(1): 61-8.
- Arce Primary Frozen Shoulder Syndrome: Arthroscopic Capsular Release. Arthrosc Tech. 2015; 4(6): e717-20.
- Romeo P, Lavanga V, Pagani D, Sansone Extracorporeal shock wave therapy in muscu- loskeletal disorders: a review. Med Princ Pract. 2014; 23(1): 7-13.
- Gerdesmeyer L, Mittermayr R, Fuerst M, Al Muderis M, Thiele R, Saxena A, Gollwitzer Current evidence of extracorporeal shock wave therapy in chronic Achilles tendinopathy. Int J Surg. 2015; 24(Pt B): 154-9.
- John L, Karin Kinesiology Taping The Essential Step-By-Step Guide. Robert Rose. 2014.
- Kase Clinical Therapeutic Applications of the Kinesio Taping Method(2nd). Tokyo. 2016.
- Hinman RS, Crossley KM, McConnell J, Bennell Efficacy of knee tape in the man- agement of osteoarthritis of the knee: blinded randomised controlled trial. BMJ. 2003 19; 327(7407): 135.
- Yeung SS, Yeung Acute Effects of Kinesio Taping on Knee Extensor Peak Torque and Stretch Reflex in Healthy Adults. Medicine. 2016; 95(4): e2615.
- Kaya E, Zinnuroglu M, Tugcu Kinesio taping compared to physical therapy modalities for the
Effects of 6 week kinesiotaping and extracorporeal shock wave therapy on the joint range of motion in patients with frozen shoulder
treatment of shoulder impingement syndrome. Clin Rheumatol. 2011; 30(2): 201-7.
- Ackermann B, Adams R, Marshall The effect of scapula taping on electromyographic activity and musical performance in profes- sional violinists. Aust J Physiother. 2002; 48(3): 197-203.
- Park C, Lee S, Yi CW, Lee The effects of extracorporeal shock wave therapy on frozen shoulder patients' pain and functions. J Phys Ther Sci. 2015; 27(12): 3659-61.
- Choi A novel approach to the treatment of shoulder pain. Kor J pain 1991; 4: 168-78.
- Pettrone FA, McCall Extracorporeal shock wave therapy without local anesthesia for chronic lateral epicondylitis. J Bone Joint Surg Am. 2005; 87(6): 1297-304.
- Lee JH, Hwang KO, Park Comparing the effects of stability exercise, ESWT, and Taping for patients with myofascial pain syndrome of
upper trapezius. J Kor Soc Phys Ther. 2012; 24(2): 82-9
- Tantawy SA, Kamel The effect of kinesio taping with exercise compared with exercise alone on pain, range of motion, and disability of the shoulder in postmastectomy females: a randomized control trial. J Phys Ther Sci. 2016; 28(12): 3300-5.
- Göksu H, Tuncay F, Borman The comparative efficacy of kinesio taping and local injection therapy in patients with subacromial impinge- ment syndrome. Acta Orthop Traumatol Turc. 2016; 50(5): 483-8.
- Aniss AM, Diener HC, Hore J, Burke D, Gandevia SC. Reflex activation of muscle spindles in human pretibial muscles during J Neurophysiol. 1990; 64(2): 671-9.
- Frederic JK, Justus Krusen's Handbook of Physical Medicine and Rehabilitation(4th ed). Saunders. 1990.





