 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Tesla
Tesla Nikola
Nikola Kayser
Kayser Fusion
FusionLateral epicondylitis: This is still a main indication for extracorporeal shockwave therapy
- Type: Free
- Introduction
The German Dr. F. Runge first described Epicondylitis humeri radialis in 1873, as “writers cramp”, and then 1883 as “Lawn Tennis elbow” in the British Journal of Sports Medicine [1]. Tennis elbow is more accurately described and understood as lateral elbow ten dinopathy d a process of failed healing affecting the common extensor tendon. Tennis elbow (also known as lateral epicondylitis) is characterized by chronic degeneration at the origin of the extensor carpi radialis brevis muscle on the lateral epicondyle of the humerus. It is usually caused by injury or overuse. Symptoms include pain, weakness and stiffness of the outer elbow. It is one of the most common tendinopathies of the upper extremity with an annual incidence of 1e3% of the total population [2]. Conservative treatments include rest, application of ice, analgesic medications with NSAR or orthopedic devices. As well physiotherapy and eccentric training and stretching are in use. Controversially dis cussed but still in use are corticosteroid injections. Over 50% of the patients go to an orthopedic surgeon, and there is a percentage of 12%, that undergo surgery after failed conservative treatment. In the beginning of the 1990s extracorporeal shock wave therapy found it's way to orthopedic treatment procedures and epi- * Corresponding author. condylitis was one of the first and obviously most successful treated Indications for ESWT. Quite a number of RCTs (Randomized Controlled Trials) were performed to prove the efficacy of the Treatment. The treatment of radial epicondylitis by ESWT even got an FDA-approval in the USA [14,15]. But there are high-quality studies, which showed not as strong results in comparison to placebo as expected and the role of ESWT for epicondylitis had to be discussed again.
According to the guidelines of ISMST (International Society for Medical Shock wave Treatment) and DIGEST (Deutschsprachige Internationale Gesellschaft für Extrakorporale Stobwellentherapie) in the following overview we want to summarize the actual known and published level-1b studies (Level of Evidence based on AHCPR 1992) with Evidence obtained from at least one randomized controlled trial. Therefor we performed a search in internet using Pubmed and Cochrane-Registers and took a look at the reference lists of articles and dissertations as well as the given talks at the international conferences of DIGEST and ISMST.We tried to compare and analyze the studies, especially on behalf of the diverging results and outcomes as well as to point out possible conflicts according to the study-design and the use of different shockwave-devices. The interpretation of the data shows to be very difficult as there is a high diversity of treatment protocols and the used scores and end-points. In earlier publications and meta-analyses these studies were excluded and smallest collections of three publications were compared or all studies are included without differentiation of all the bias of generators, local anesthesia and so on. We therefor wanted to include the published level-1b-Studies and rated them due to the clinical use and guidelines of ISMST and DIGEST.
- A number of studies with negative results were published in the years of 2002 to 2008
Crowther et al. [3] published in 2002 a controlled trial shockwave-therapy vs. local steroid injection with 93 patients with a follow-up after 6 weeks and 3 months. After three months, 84% of patients in group 1 were considered to have had successful treat ment by a single injection of 20 mg triamcinolone with lignocaine compared with 60% in group 2 receiving 2000 shock waves in three sessions at weekly interval.
The conclusion of the authors showed in the medium term local injection of steroid being more successful and 100 (??) times less expensive than ESWT in the treatment of tennis elbow. However local injections of steroids have to be discussed as harmful in the long term and therefore seems not to be a treatment option. Taking a closer look to the study the randomization has to be criticized as a number of patients randomized to receive the injection refused the injection and therefore the patients receiving the injection are a positive-selection. In our opinion Crowther et al. even showed a positive result for ESWT but the study has to be excluded as comparison to cortico steroids in chronic tissue disorders seems to be inadequate and the randomization process was incorrect.
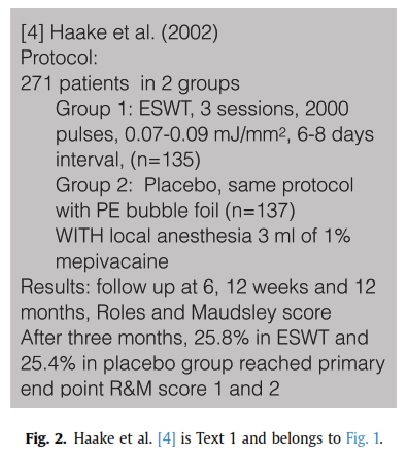
In one of the biggest studies Haake et al. [4] randomized 271 patients in a multi center study in 2002 comparing ESWT vs. placebo.
Results: follow up at 6 weeks, 12 weeks and 12 months, Roles and Maudsley score (see Figs. 1 and 2).
After three months, 25,8% in ESWT and 25,4% in placebo group reached the primary end point in the Roles and Maudsley score “1 or 2” out of 4 and no requirement for additional treatment. Conclusions of the authors “Extracorporeal shockwave therapy as applied in the present study is ineffective for the treatment of chronic lateral
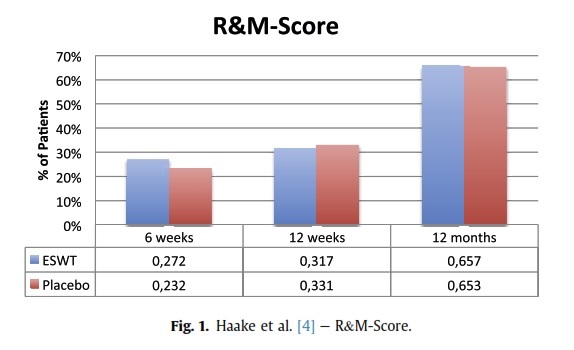
epicondylitis. Six weeks, three months, and one year after extra corporeal shock wave therapy with 3 2000 pulses and positive energy flux density (EDþ) of 0,07 to 0.09 mJ/mm2 and use of local anesthesia, we detected no relevant difference in the clinical suc cess rate compared with that in a placebo therapy group.”
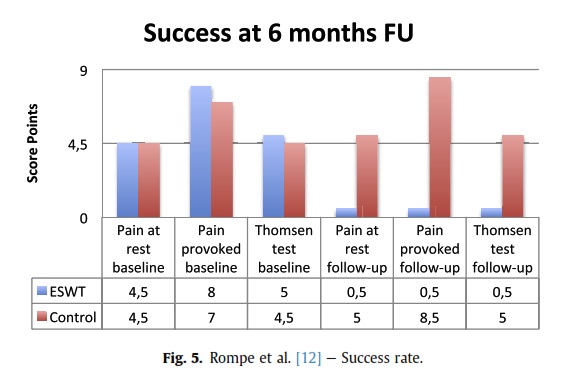
In an additional follow-up after one year, the authors found an improvement in two-thirds of the patients in both groups. The study-design unfortunately includes the use of local anes thesia, very low intensities and as a multi center-study the shock wave-generators were not similar and different intensities were in use as revealed by the authors. According to Labek et al. [5] the use of local anesthesia shows a negative influence on shock wave treatment and might have impaired this study. Local anes thesia inhibits the C-fibre-activity and substantially alters the biological response to ESWT (see Fig. 5).
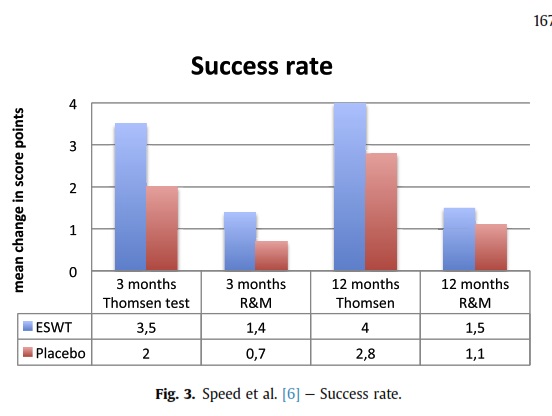
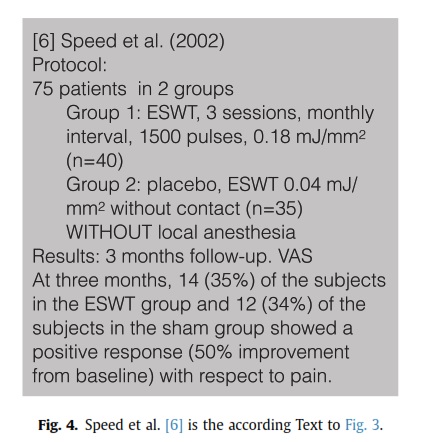
In an often quoted study Speed et al. [6] showed 2002 no sig nificant effect of ESWT in lateral epicondylitis within a short period of 3 months (Figs. 3 and 4).
Results: 3 months follow-up. VAS.
At three months, 14 (35%) of the subjects in the ESWT group and 12 (34%) of the subjects in the sham group showed a positive response (50% improvement from baseline) with respect to pain. Conclusions of the authors
There appears to be a significant placebo effect of moderate dose ESWT in subjects with lateral epicondylitis but there is no evidence of added benefit of treatment when compared to sham therapy.
In comparison both groups show a low positive effect to the treatment, but the sham group was treated with a minimal Energy flux density of 0.04 mJ/mm. No matter the little amount of energy this controverts the principle of a sham group.
Melikyan et al. [7] showed in 2003 no difference between ESWT and placebo using a foam pad and even showed about the
same number of patients going to surgery after remaining pain within the two groups. All patients improved significantly over time, regardless of treatment but still the authors had to state that this study showed no evidence that extracorporeal shockwave therapy for tennis elbow is better than placebo.
Chung et al. [8] who performed in 2004 a controlled trial with 59 patients in two groups using an electromagnetic shockwave device compared to a group with an intervening air pad to extin guish the shockwave-effect. All patients received additionally a forearm-stretching program. Success rates in the sham and active therapy groups were 31% and 39%, no significant difference was detected between groups within the short follow-up of only 8 weeks. Still it has to be mentioned, that both groups showed within the short FU an improvement in quality of life and grip-strength of 7.4 respectively 6.8 kg. This study therefore is limited due to a variable amount of energy flux utilized and the short duration of follow-up. Lebrun et al. [9] performed a study including 60 patients in 2005.
The results after 8 weeks follow-up in VAS showed the pro portions of treatment successes in the sham ESWT and the active ESWT with 31% and 39% (p ¼ 0.533).
In the conclusions of the authors a low-dose ESWT did not have a clinically important effect in reducing pain, improving quality of life, or increasing pain-free grip strength in middle-aged patients with previously untreated unilateral or bilateral lateral epi condylitis. Here as well the short follow-up has to be criticized.
Staples et al. [10] in 2008 showed positive effects but no differences within the two groups. Follow-up was investigated at 3 weeks, 3 months and 6 months. The groups did not differ on de mographic or clinical characteristics at baseline and there were significant improvements in almost all outcome measures for both groups over the 6-month follow-up period, but there were no dif ferences between the groups even after adjusting for duration of symptoms. The authors therefore state, that this study found little evidence to support the use of ESWT for the treatment of lateral epicondylitis and is consistent to recent systematic reviews of ESWT for lateral epicondylitis that have drawn similar conclusions. Same as in the study of Speed et al. [6], Staples performs a “sub therapeutic” dose of ESWT in the sham group.
- Studies with positive results in RCTs could be found in the years 1996 to 2012
Mehra et al. [11] performed in 2003 a controlled trial to show the use of a mobile lithotripter in the treatment of tennis elbow and plantar fasciitis with a follow-up at 6 months, assessing a VAS.
In the treatment groups, a final pain score at six months post treatment showed significant improvement (three or more points) in 78% of patients with tennis elbow.
Conclusion of the authors:
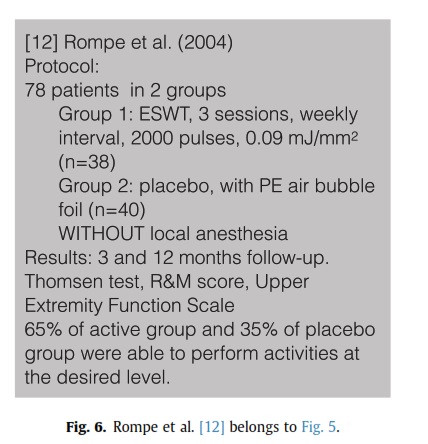
The mobile lithotripter is an effective way of treating tennis elbow and plantar fasciitis but warrants further larger studies. Rompe et al. [12] performed a placebo-controlled trial using repetitive low-energy shock wave treatment in 2004 due to the conflicting evidence regarding ESWT for chronic tennis elbow. The treatment was performed with patients with recalcitrant MRI confirmed tennis elbow of at least 12 months duration and the follow-up was performed at 3 and 12 months. Thomsen test, Roles and Maudsley score, Upper Extremity Function Scale were used to score the patients (see Figs. 5 and 6).
65% of the active group and 35% of placebo group were able to perform activities at the desired level and achieved at least 50%
reduction of pain.
The conclusions of the authors agreed, that there is a significant benefit of low-energy ESWT as applied when compared to sham treatment for tennis elbow 3 months after intervention. There is a considerable placebo effect of low-energy ESWT in patients with chronic lateral epicondylitis.
Already in 1996 Rompe et al. [13] showed similar positive results in a RCT with two groups treating lateral epicondylitis. As well in 2004 Levitt et al. [14] presented a study at the AAOS Annual Meeting including 183 patients using an electrohydraulic device and a Styrofoam block showing a positive outcome as an FDA-approval study.
Success after 8 weeks could be shown in 51% of the patients in the ESWT-group and 37% in the placebo group in a self-assessment and VAS.
Pettrone et al. [15] performed as well a RCT leading to an FDA approval in 2005 with a 12 weeks follow-up in the scores of Thomsen test, pain score, and grip strength including 114 patients (see Figs. 7 and 8).
61% (34) of 56 patients in the active treatment group compared with only 29% (17) of 58 patients in placebo group had >50% reduction of pain in Thomsen test. Likewise the functional activity scores, activity-specific evaluation and overall impression of the disease state showed significant improvement in the treatment group.
Extracorporeal shockwave therapy as utilized in the current study, without the use of local anesthesia is safe and effective treatment of chronic lateral epicondylitis as stated by the authors.
In patients who have had failure of conventional treatment of lateral epicondylitis, shockwave therapy can significantly improve the pain scores, functional scores, and the subjective impression of the disease state.
Additionally in a follow-up after 12 months the improvement persisted after ESWT in those patients that were followed (see Fig. 7).
Spacca et al. [16] could display same good results in 2005 using a radial shockwave-device, (see Figs. 9 and 10). Comparing the same parameter before and after treatment within each group of each 31 patients, a statistically significant improvement is shown in the study group. The authors state that the use of radial shockwave therapy allowed a decrease of pain, and functional impairment, and an increase of the pain free grip strength test, in patients with tennis elbow. The RSWT is safe and effective and must be considered as a possible therapy for the treatment of patients with tennis elbow.
Radwan et al. 2007 [17] performed a controlled trial comparing ESWT to surgery. Resistant tennis elbow: shock-wave therapy versus percutaneous tenotomy with 12 weeks and 12 months follow-up. At three months, the success rates, defined as Roles and Maudsley score: excellent and good, were 74,1% of patients in the tenotomy group and 65,5% of ESWT patients.
The success rate (Roles and Maudsley score: excellent and good) at three months in the ESWT group was 65,5% and in the tenotomy group was 74,1%. ESWT appeared to be a useful noninvasive treat ment method that reduces the necessity for surgical procedures. (see Figs. 2, 4, 6, 8e10).
findings laterality different to the dominant limb and repeated shockwave treatments are prognostic factors in an unsuccessful therapy, while being male and a high body mass index are factors for success.
As well Trentini et al. [24] as well in 2015 show ESWT for EHR to be a valuable and safe solution, representing a definitive treatment in the majority of patients. But patients refractory to a 3-to 4- session ESWT cycle have lower chances of positive response after further ESWT cycles.
Furia [25] 2005 investigated the efficacy and safety of ESWT in 36 patients with chronic lateral epicondylitis showing a significant improvement in the mean VAS with excellent or good outcomes on the Roles & Maudsley scale in 77.8%, stating ESWT as an effective treatment for EHR. No significant complications were observed and the worker's compensation status did not affect outcomes.
Rating all the studies we see that only a little number of studies showing negative results [3,6and7] and a veritable number of studies showing positive results [12,13,15,16,17 and 19] are compatible to the guidelines of ISMST and DIGEST.
Taking a look on the present guidelines for the treatment of tennis elbow Theis et al. [26] in 2004 showed that surgery is not indicated before repetitive low-energy ESWT has been applied.
- Overall conclusion
We included in our Overview only studies with level EBM 1b, which were performed close to the guidelines of the ISMST (www. ismst.com) and the DIGEST (“http://www.digest-ev.de).
The current evidence base seems to be adequate to support the use of ESWT for lateral epicondylitis with symptoms beyond three months. Of course further research should be focussed on the best treatment regimes but efficacy has been well demonstrated. In our opinion there is a majority of studies with an evident proof of ef ficacy for ESWT in the treatment of epicondylitis. Even studies with platinum evidence had systematic faults and could not be taken for this analysis.
ESWT should only be used without local anesthesia, for chronic indications, the follow-up should be more than 3 months, better one year, and it is only possible to compare shockwave devices with the same shockwave generation principle. Further research should focus on best treatment regimes, but the current evidence base seems to be adequate to support the use of ESWT for Epicondylitis humeri radialis with symptoms beyond 3 months.
Therefor in our opinion the qualitative and quantities analysis of studies for the treatment of epicondylitis radials by ESWT is positive!
References
[1] F. Runge, Zur Genese und Behandlung des Schreibekrampfes, Berl. Klin. Wochenschr. 21 (1873) 245e248.
[2] D. Richter, A. Ekkernkamp, G. Muhr, Die extrakorporale Stoßwellentherapie e ein alternatives Konzept zur Behandlung der Epicondylitis humeri radiales, Orthop€ade 24 (1995) 303e306.
[3] M.A.A. Crowther, G.C. Bannister, H. Huma, G.D. Rooker, A prospective, rand omised study to compare extracorporeal shock-wave therapy and injection of
steroid for the treatment of tennis elbow, J. Bone Jt. Surg. Br. 84 (5) (2002) 678e679.
[4] M. Haake, I.R. Konig, T. Decker, C. Riedel, M. Buch, H.-H. Muller, Extracorporeal shock wave therapy in the treatment of lateral epicondylitis : a randomized multicenter trial, J. Bone Jt. Surg. Am. 84-A (11) (2002) 1982e1991.
[5] G. Labek, V. Auersperg, M. Ziernhold, N. Poulios, N. B € ohler, Ein € fluss von Energie und Lokalinfiltration auf klinischen Outcome nach ESWT bei plan tarem Fersensporn. Vortrag beim 2, Drei-Lander-Treffen der € Osterreichischen, € Schweizerischen und Deutschen Gesellschaften für Orthopadische Extra- € korporale Stoßwellentherapie. Linz, 19.e20.04, 2002.
[6] C.A. Speed, D. Nichols, C. Richards, H. Humphreys, J.T. Wies, S. Burnet, B.L. Hazleman, Extracorporeal shock wave therapy for lateral epicondylitisea double blind randomised controlled trial, J. Orthop. Res. 20 (5) (2002) 895e898.
[7] E.Y. Melikyan, E. Shahin, J. Miles, L.C. Bainbridge, Extracorporeal shock-wave treatment for tennis elbow. a randomised double-blind study, J. Bone Jt. Surg. Br. 85 (6) (Aug 2003) 852e855.
[8] B. Chung, J.P. Wiley, Effectiveness of extracorporeal shock wave therapy in the treatment of previously untreated lateral epicondylitis: a randomized controlled trial, Am. J. Sports Med. 32 (7) (2004) 1660e1667.
[9] C.M. Lebrun, Low-dose extracorporeal shock wave therapy for previously untreated lateral epicondylitis, Clin. J. Sport Med. 15 (5) (2005) 401e402. [10] M.P. Staples, A. Forbes, R. Ptasznik, J. Gordon, R. Buchbinder, A randomized controlled trial of extracorporeal shock wave therapy for lateral epicondylitis (tennis elbow), J. Rheumatol. 35 (10) (2008 Oct) 2038e2046.
[11] A. Mehra, T. Zaman, A.I.R. Jenkin, The use of a mobile lithotripter in the treatment of tennis elbow and plantar fasciitis, Surgeon 1 (5) (Oct 2003) 290e292.
[12] J.D. Rompe, J. Decking, C. Schoellner, C. Theis, Repetitive low-energy shock wave treatment for chronic lateral epicondylitis in tennis players, Am. J. Sports Med. 32 (3) (2004) 734e743.





