 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Tesla
Tesla Nikola
Nikola Kayser
Kayser Fusion
FusionCombined physiotherapy and education is efficacious for chronic low back pain
- Type: Free
Manual therapy, exercise and education target distinct aspects of chronic low back pain and probably have distinct effects.This study aimed to determine the efficacy of a combined physiotherapy treatment that comprised all of these strategies. Byconcealed randomisation, 57 chronic low back pain patients were allocated to either the four-week physiotherapy program ormanagement as directed by their general practitioners. The dependent variables of interest were pain and disability.Assessors were blind to treatment group. Outcome data from 49 subjects (86%) showed a significant treatment effect. Thephysiotherapy program reduced pain and disability by a mean of 1.5/10 points on a numerical rating scale (95% CI 0.7 to 2.3)and 3.9 points on the 18-point Roland Morris Disability Questionnaire (95% CI 2 to 5.8) , respectively. The number needed totreat in order to gain a clinically meaningful change was 3 (95% CI 3 to 8) for pain, and 2 (95% CI 2 to 5) for disability. Atreatment effect was maintained at one-year follow-up. The findings support the efficacy of combined physiotherapy treatmentin producing symptomatic and functional change in moderately disabled chronic low back pain patients.[Moseley L (2002):Combined physiotherapy and education is efficacious for chronic low back pain.Australian Journal ofPhysiotherapy 48: 297-302]

Introduction
Chronic low back pain is a multifactorial phenomenon andit is not surprising that many therapeutic approaches exist.Some approaches are ineffective but manual therapy,specific muscle training, cognitive behavioural therapy andmultidisciplinary pain management programs have all beensupported. Distinct approaches tend to target distincteffects. For example, manual therapy (mobilisation and/ormanipulation of the lumbar spine) is effective in reducingpain (Andersson et al 1999, Cherkin et al 1998, Triano et al1995), and specific exercise programs which aim to restorenormal function of the trunk muscles are effective inreducing disability and increasing performance at least inmildly disabled patients (Mannion et al 1999, O’Sullivan etal 1997). Although they may be effective in producingbenefit across outcome domains, these approaches do notdirectly address psychosocial aspects of pain. In somepatients, such aspects are thought to be enduring barriers toimprovement. These patients may obtain more benefit fromprograms that directly address cognitive and behaviouralaspects of pain.Multidisciplinary pain management programs, whichusually focus on cognitive and behavioural aspects, areprimarily effective in reducing disability, promoting self-efficacy and normalising pain cognitions (Guzman et al2001, McQuay et al 1997). Not all programs are alike;more intensive programs, although more expensive, appearto be more effective (Guzman et al 2001, Williams et al1996). The fact that they require substantial personnel andeconomic resources is a limitation of multidisciplinary programs. An alternative way to target cognitive andbehavioural aspects of chronic low back pain is through thetargeted provision of information. Education in this mannerattempts to effect change through reconceptualisation ofthe problem. Employing an education approach may appear surprisingbecause for some time, there has been a consensus thatthere is no clinically important effect of educationprograms for chronic low back pain (Cohen et al 1994).Reviews on education-based back schools appearconvincing (Koes et al 1994), however, recent evidencesuggests that the lack of effect is probably due to the typeof information that has been presented. Studies that haveemployed an approach to education that emphasisescognitive-behavioural (Burton et al 1999, Linton andAndersson 2000, Symonds et al 1995) orneurophysiological (Moseley et al 2001) aspects havereported reduced disability, reduced health care utilisation,normalisation of pain cognitions, and increased self-efficacy.
Manual therapy, specific exercise training and targetededucation all seem to promote therapeutic success throughtargeting distinct aspects of chronic low back pain.Although each of these strategies is broadly encompassedwithin the domain of physiotherapy, the effect of acombined physiotherapy treatment that consists of all threestrategies is not known. The aim of this study was todetermine the effect of such a combined physiotherapytreatment on functional and symptomatic parameters ofmoderately disabled patients with chronic low back pain.
Methods
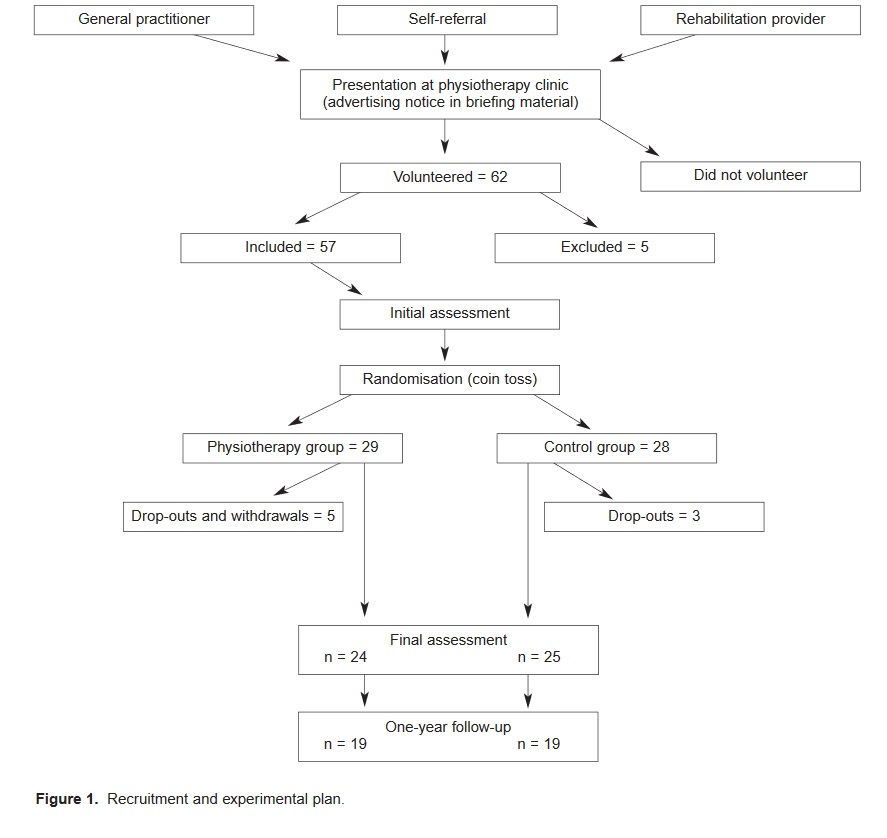
Experimental design This study was a randomisedcontrolled trial with repeated measures comparison ofmeans. The study was approved by the InstitutionalMedical Research Ethics Committee and all proceduresconformed with the Declaration of Helsinki.Subjects Sixty-two subjects volunteered for the study byresponding to a note that advertised the project. The notewas included in the material given to each patient on initialattendance at participating physiotherapy clinics or thereferring general practitioner. Subjects were included if theprimary reason for presentation was a history of low backpain of greater than two months. Subjects were excluded ifthey were unable to understand, read and speak English,had worsening neural signs, had any neurological ororthopaedic condition that would interfere with treatment,or were awaiting surgery. Five subjects were excluded. While each subject was undertaking the initial assessment,an independent person allocated them to experimentalgroup using a coin toss. This strategy ensured thatallocation was concealed from the subjects until after initialassessment, and from the assessors throughout the study.Twenty-nine and 28 subjects were allocated to thephysiotherapy and control groups respectively. Figure 1presents the recruitment strategy and experimental plan.
Experimental protocol The following items were used asoutcome measures: the 18-item Roland Morris DisabilityQuestionnaire (RMDQ; Roland and Morris 1983) and the0-10 Numerical Rating Scale (NRS) for pain (“How wouldyou rate your low back pain, on average, over the last threedays?”). Initial and final assessment was performed by thesame two investigators, who were not otherwise involved inthe study and were blinded to experimental group. One-year follow-up data were collected via telephone byseparate assessors who were also blinded to experimentalgroup. The properties of the RMDQ and the NRS for painare thought to be maintained when administered over thephone (Cherkin et al 1998). A further question estimatedthe number of health visits for low back pain over thecourse of the follow-up period: “Since your assessment on[date of final assessment], how many times have youconsulted a health care professional for your low backpain?”
Treatment protocol Each subject received twophysiotherapy treatments per week for four weeks. Manualtherapy treatment involved symptom managementaccording to the discretion of the treating physiotherapist,who chose from spinal mobilisation/manipulation, softtissue massage, and muscle and neuromeningealmobilisation techniques, but not electrophysicalmodalities.
Each subject participated in specific trunk muscle trainingboth on an individualised level on two occasions per weekand through a standardised home-exercise program. Thisprogram was conducted according to the protocol described by Richardson and colleagues (Richardson andJull 1995). Subjects were instructed to maintain the homeprogram indefinitely. Compliance with the home programwas not assessed. Each subject participated in a one-hour education session,once per week for four weeks. The education session was ina one-to-one seminar format, was conducted by anindependent therapist, and focused on the neurophysiologyof pain with no particular reference to the lumbar spine. Inaddition, the subjects completed a short workbook whichconsisted of one page of revision material and threecomprehension exercises per day for 10 days.Subjects in the control group received ongoing medicalmanagement as advised by their general practitioner. Thesesubjects were also advised not to seek physiotherapytreatment during the data collection period. Subjects in thecontrol group were questioned after the final assessment asto what intervention, if any, they had since initialassessment and how many visits to the general practitionerthey had made for their low back pain.Analysis Two-factor repeated measures ANOVAs (groupxtime) were used to identify a treatment effect on thedependent variables at final assessment and at one-yearfollow-up. Numerical Rating Scale and RMDQ were thedependent variables. Because two separate ANOVAs wereused in the analysis, the probability of a Type 1 error for thestudy was elevated. To adjust for this, a Bonferronicorrection yieldedα= 0.025. Analysis was by intention totreat.
For those dependent variables in which the group xtimeinteraction was significant, treatment affects wereestimated from the difference in group means. For NRSand RMDQ, the number needed to treat (NTT) in order togain a clinically significant change was also determined.The threshold for a clinically significant change in NRSand RMDQ was set a-priori at 2 points and 4 points,respectively. These values were selected according toestimates in the literature, (eg Stratford et al 1994, Turk andMelzack 1992).
Results
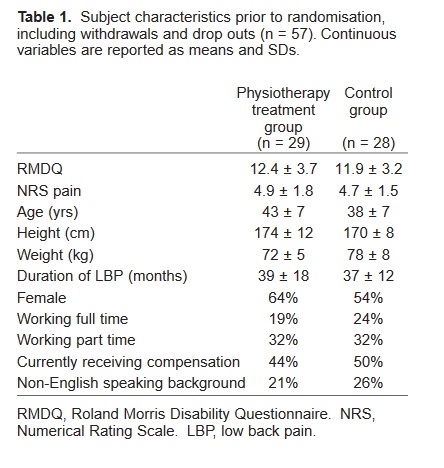
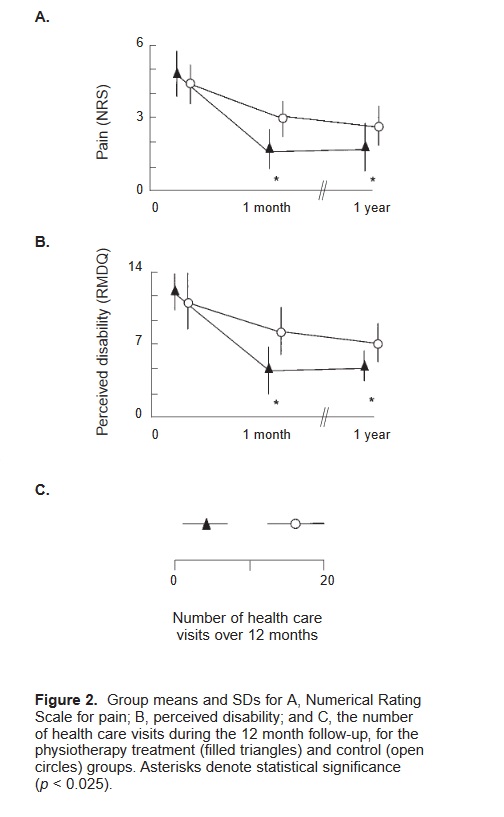
Subject details Table 1 shows the subject characteristics.There were no pre-treatment differences between thegroups in any of these measures or in the dependentvariables (p> 0.31). On final assessment, the mean numberof visits to the general practitioner was 4 (SD 2). Eighteenof the subjects in the control group indicated that they hadbeen prescribed physical exercises by their generalpractitioner previous to the initial assessment, but only six subjects had these exercises reviewed during the datacollection period. Six subjects indicated that they hadreceived weekly manipulations from their generalpractitioner and nine subjects indicated that their pain reliefmedications had been increased or altered during the datacollection period. Two control subjects received weeklyanalgesic injections during the data collection period.Pain and disability Final assessment was performed 29 ±6 days after the initial assessment. There was a meanreduction of 2.9/10 and 1.4/10 on the NRS for pain, and8.2/18 and 4.3/18 points on the RMDQ, for thephysiotherapy treatment and control groups respectively(Figure 2). Thus, the mean improvement effected byphysiotherapy treatment was 1.5 points on the NRS forpain (95% CI 0.7 to 2.3) and 3.9 points on the RMDQ(95% CI 2.0 to 5.8). The repeated measures ANOVAsindicated a significant treatment effect on NRS and RMDQ(p<0.01 for both). The number needed to treat (NNT) togain a clinically significant change was 3 (95% CI 2 to 8)for the NRS and 2 (95% CI 2 to 5) for the RMDQ. Twelve-month follow-up Nineteen subjects in each group(67% of total sample) were contactable at one year (mean ±SD = 352 ± 28 days) for follow-up. There were significanttreatment effects on NRS and RMDQ, and on the number ofhealth care visits for low back pain during the follow-upperiod (Figure 2). The treatment effect was 1.9 for pain(95% CI 1 to 2.8) and 3.9 points on the RMDQ (2.3 to 5.8)corresponding to numbers needed to treat of 2 (95% CI 1 to4) and 2 (1 to 3) respectively. During the one year since finalassessment, subjects from the physiotherapy group made amean ± SD 3.6 ± 2 health care visits for their low back pain,which was fewer than the control group, who attended amean ± SD 13.2 ± 5 health care visits (p< 0.001). Thus theeffect of treatment was to reduce the number of health carevisits by a mean of 9.6 (95% CI 6.9 to 11.9).Withdrawals, dropouts and side effects Four and threesubjects, from the physiotherapy group and control grouprespectively, dropped out of the study and could not becontacted. One subject from the physiotherapy groupwithdrew due to urgent surgery unrelated to low back pain.Twenty-four and 25 subjects completed the physiotherapyand control programs respectively. The pre-treatment datafor those subjects included in the follow up showed nodifferences between the experimental groups (t-test, p> 0.21).
Discussion
These findings show that a combined physiotherapytreatment consisting of manual therapy, specific exercisetraining, and neurophysiology education is effective inproducing functional and symptomatic improvement inchronic low back pain patients. This is evidenced by asignificant treatment effect and substantial effect size forpain and disability, both of which appear to be maintainedfor at least one year.
The effectiveness of the physiotherapy program is substantiated by the NNT analysis. One advantage of theNNT is that it provides a clinically relevant indication ofthe number of patients that need to be treated for one morepatient to achieve a particular therapeutic target. In short,an NNT of 1 suggests that the desired target is achieved inevery patient in the treatment group but in no patient in thecontrol group. Thus, the closer the NNT is to 1, the betterthe treatment is at achieving the targeted outcome. TheNNTs in the current work were 3 (pain) and 2 (disability),which are consistent with recommendations in theliterature that stipulate that, for chronic pain, NNTs of 2 or3 are indicative of an effective intervention (McQuay et al1997)
The current results suggest that the combinedphysiotherapy treatment is probably more effective than thecomponents administered in isolation. This is primarilyevidenced by the fact that most of the effects of soletreatments reported in the literature are small, particularlyin those studies that involved subjects with high initialdisability levels. For example, manipulation has beenreported to produce effects of 2/10 and 3 RMDQ points(Cherkin et al 1998), 1.6/10 (Andersson et al 1999) and2.5/10 (Triano et al 1995); exercise has been reported toproduce effects of 1.2/10 and 2.9 RMDQ points (KlaberMoffett et al 1999); and education has been reported toproduce effects of (1/10 and 2.5 RMDQ points (Cherkin etal 1998), 0/10 and 1 RMDQ point (Moseley et al 2001).Even so, chronic low back pain is heterogeneous andsubjects vary across studies in their chronicity, painintensity, functional level and pain impact. This means thatthe validity of a comparison between the current work andother studies is limited. For this study, it is ultimately impossible to isolate thecontribution that each component treatment made to theoutcome of the combined treatment. In future studies,teasing out the relative contribution of componentstrategies to the therapeutic effect may allow conclusionsabout the mechanisms involved. This may, in turn, enhancethe efficacy of combined physiotherapy treatments andpermit targeting of sub-groups of patients with chronic lowback pain.Considering the high economic cost of chronic low backpain, targeting of sub-groups may be beneficial. This studysuggests that a combined physiotherapy treatment is a costeffective strategy when targeted at moderately disabledpatients with chronic low back pain; based on A$60.00 persession, the estimated cost of the combined treatment wasA$720, which compares favourably with multidisciplinarypain management programs that can cost in the order ofA$4000 (Moseley 1997, unpublished data). Importantly,however, the combined physiotherapy treatment may beneither cost-effective nor efficacious in more disabledpatients with chronic low back pain or in other sub-groupsof patients with chronic pain. Psychosocial factors arethought to be more important in some sub-groups and thereis considerable evidence in support of more intensive,albeit more expensive, strategies for such patients (Guzmanet al 2001, Morley et al 1999). One aspect of the current study that is open to criticism isthe lack of a robust control group. Although “ongoingmedical management” is used widely and generallyaccepted as suitable for clinical trials, it does notadequately remove many sources of bias. By and large, thisshortcoming is ignored in the relevant literature (eg Bendixet al 1997, Deyo 1996, Hides et al 1996, Laclaire et al1996, O’Sullivan et al 1998, van der Heijden et al 1995).However, non-treatment factors such as patientexpectations (Carosella et al 1994, Montgomery andKirsch 1997), health provider expectations (Gracely et al1985, Shapiro et al 1954), patient-provider rapport (Egbertet al 1964), therapist enthusiasm and perceived level of expertise (Nordin et al 1998, Shapiro and Shapiro 1984)are all considered to contribute to therapeutic effect. Bias may also be introduced by the Hawthorne effect,which is caused by knowledge that one is participating in aresearch study (Parson 1974). However, if the Hawthorneeffect varies according to how much the subject isparticipating (this certainly seems reasonable), then in thepresent work, the Hawthorne effect would have beengreater in the physiotherapy group. Thus, although thecurrent findings appear potent, further trials incorporatinga more robust control group probably are required tosubstantiate the results of the current study. One source of bias that may limit the external validity ofthis work is selection bias introduced by the exclusioncriterion that subjects have an ability to read, speak andunderstand English. Although 28% of subjects were from anon-English speaking background, broad application of thecurrent findings to linguistically diverse chronic low backpain patients would appear problematic. Notwithstanding the potential limitations of the currentwork, the results strongly suggest that the combinedphysiotherapy treatment, consisting of manual therapy,specific exercise training, and neurophysiology education,is effective in producing functional and symptomaticimprovement in chronic low back pain patients. The effectis maintained at 12 months post-treatment and patientssubsequently seek substantially fewer health care visitsthan those under ongoing medical care. The findingspresented here are important because they support thelong-term efficacy of this approach for a problematicpatient group: moderately disabled patients with chroniclow back pain.
References
- Andersson GBJ, Lucente T, Davix AM, Kappler RE, LiptonJAand Leurgans S (1999): A comparison of osteopathicspinal manipulation with standard care for patients withlow back pain.New England Journal of Medicine341: 1426-1431.
- Bendix AF, Bendix T, Lund C, Kirkbak S and Ostenfeld S(1997): Comparison of three intensive programs forchronic low back pain patients: a prospective,randomized, observer-blinded study with one-year follow-up.Scandinavian Journal of Rehabilitation Medicine29: 81-89.
- Burton AK, Waddell G, Tillotson KM and Summerton N(1999): Information and advice to patients with back paincan have a positive effect. A randomized controlled trial ofa novel educational booklet in primary care.Spine24: 2484-2491
- Australian Journal of Physiotherapy 2002 Vol. 48302Cherkin DC, Deyo RA, Battie M, Street J and Barlow W(1998): A comparison of physical therapy, chiropracticmanipulation, and provision of an educational booklet forthe treatment of patients with low back pain.New EnglandJournal of Medicine 339: 1021-1029





