 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Tesla
Tesla Nikola
Nikola Kayser
Kayser Fusion
FusionPhysiotherapy management of knee osteoarthritis
- Type: Free
Abstract
Knee osteoarthritis (OA) is a prevalent chronic joint disease causing pain and disability. Physiotherapy, which encompasses a number of modalities, is a non-invasive treatment option in the management of OA. This review summarizes the evidence for commonly used physiotherapy interventions. There is strong evidence to show short-term beneficial effects of exercise on pain and function, although the type of exercise does not seem to influence treatment outcome. Delivery modes, including individual, group or home exercise are all effective, although therapist contact may improve benefits. Attention to improving adherence to exercise is needed to maximize outcomes in the longer-term. Knee taping applied with the aim of realigning the patella and unloading soft tissues can reduce pain. There is also evidence to support the use of knee braces in people with knee OA. Biomechanical studies show that lateral wedge shoe insoles reduce knee load but clinical trials do not support symptomatic benefits. Recent studies suggest individual shoe characteristics also affect knee load and there is current interest in the effect of modified shoe designs. Manual therapy, while not to be used as a stand-alone treatment, may be beneficial. In summary, although the research is not equivocal, there is sufficient evidence to indicate that physiotherapy interventions can reduce pain and improve function in those with knee OA.
Key words: braces, exercise, insoles, knee, management, manual therapy, osteoarthritis, patellar taping, physical therapy, physiotherapy.
INTRODUCTION
Osteoarthritis (OA) is a chronic joint disease, which commonly affects the knee. OA can cause pain, stiffness, swelling, joint instability and muscle weakness, all of which can lead to impaired physical function and reduced quality of life. Non-pharmacological interventions to improve symptoms are advocated and there is growing recognition that physiotherapy treatments can play an important role in the multidisciplinary management of patients with knee OA. This article will briefly outline the evidence for the effectiveness of several common physiotherapy treatments, including exercise, taping, bracing, insoles and shoes and manual therapy, in reducing knee OA symptoms. While some of the treatments also have the potential to slow structural disease progression by virtue of their effects on knee load, discussion of this is beyond the scope of this short review.
EXERCISE
Given the large body of evidence demonstrating the beneficial clinical effects of exercise in people with knee OA of varying severity, exercise therapy is regarded as the cornerstone of conservative management and is recommended by clinical guidelines.1–6 Importantly, exercise has similar effect sizes to simple analgesic and non-steroidal anti-inflammatory drugs, but is accompanied by few contraindications or adverse effects, unlike drugs and surgery.2 A summary of evidence-based recommendations for exercise in knee OA are shown in Table 1.
A recent Cochrane review identified 32 trials investigating a variety of land-based therapeutic exercise programs.7 Results of a meta-analysis showed mean treatment benefits for both knee pain and physical function. Although there is less robust research into the effects of aquatic exercise, a small-to-moderate effect on function and a small-to-moderate effect on quality of life have been reported in another relatively recent Cochrane review.8 Typical physiological changes as a result of an effective exercise regime may include improvements in muscle strength, neuromuscular control, range of motion, joint stability and fitness. Strengthening exercise is commonly recommended. Patients with knee OA tend to have reduced muscle strength as a consequence of reductions in physical activity and pain inhibition.9–12 The quadriceps are the largest group of muscles crossing the knee joint and have the greatest potential to generate and absorb forces at the knee. Many clinical studies have shown
consistent improvements in knee extension strength after training, as well as reductions in pain and physical disability in people with knee OA.7,13 However, no particular method of strength training has been determined to be superior to others.13 Recent studies have also highlighted the role of hip muscle strengthening in knee OA.14–16 Results suggest that improvements in pain and function can be gained by increasing hip muscle strength.16 This may prove particularly useful when pain limits specific knee exercises. Although not well studied, local mechanical forces such as knee malalignment may influence the symptomatic response to strength training.17 This highlights the importance of individual assessment and management strategies for patients with knee OA.
At this stage, there is no evidence to support the effectiveness of one specific form of exercise over another,7 although a combination of strengthening, aerobic and functional exercise is recommended. Exercise may also be delivered via individual treatments, supervised group classes or performed at home. It appears that all three modes of exercise delivery are effective in reducing symptoms7,18; however, therapist contact may improve outcomes.7,18 Another consideration is the frequency and duration of an exercise program. Most exercise guidelines would suggest a physiological response can be attained with as few as 2–3 exercise sessions per week, and exercise programs in individuals with knee OA have led to improvements in symptoms after 8–12 weeks.19 However, the optimal exercise dosage is yet to be determined and should be individualized to each patient.
Adherence to exercise is often good in the first few months of commencing an exercise program but declines rapidly over time. Patient adherence is a key factor in determining improvements in outcome from exercise therapy in patients with knee OA. Adherence is improved when patients receive attention from health professionals,18 believe in the effectiveness of the intervention and understand the pathogenesis of knee OA.20 Self-efficacy, or one’s belief in their own ability to perform tasks, is also associated with greater adherence and better outcomes.21 Thus, strategies to maximize adherence to exercise should be incorporated, including educating patients about the disease and benefits of exercise, long-term monitoring review by a clinical exercise professional, regular follow-up or booster sessions, use of pedometers or a self-reported diary and support from family and friends.22
TAPING
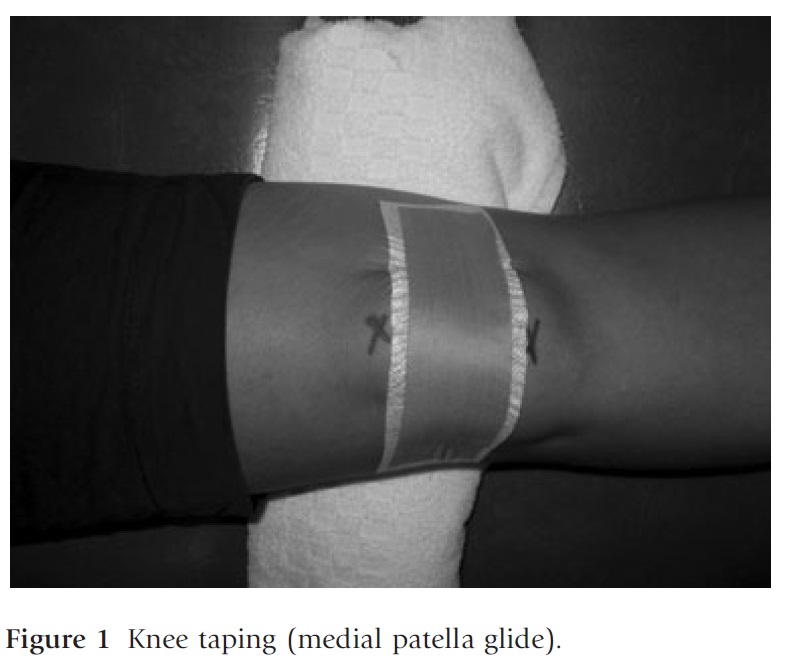
Taping the knee, in particular the patella, is a physiotherapy treatment strategy recommended in the management of knee OA by some clinical guidelines.5,6 Knee taping involves the application of adhesive rigid strapping tape to the patella and/or associated soft tissue structures (Fig. 1). Taping aims to realign the patella so as to reduce patellofemoral joint (PFJ) stress and to unload painful soft tissues around the knee joint, with the ultimate intention of reducing knee pain. Immediate and short-term reductions in pain have been demonstrated in several randomized controlled trials in patients with knee OA both with and without OA involvement of the PFJ.23–25 While it might be expected that the pain-relieving effects of tape are confined to when the tape is worn, one study found that benefits were still present 3 weeks following tape removal.25
The mechanism by which taping reduces pain is not clear, but may include changes in patellar alignment26 and enhanced function and activation of muscles.27 However, the latter has only been demonstrated in patients with patellofemoral pain and is yet to be confirmed in those patients with OA.28
There are several practical aspects to knee taping that must be considered. Skin care is important to minimise the risk of adverse effects. Patients should initially be screened to ensure they are appropriate for taping and hypoallergenic undertape should be used to protect skin from direct contact by the rigid strapping tape that is used to realign the patellar and unload soft tissues. The majority of skin damage is caused by frequent removal of tape. Thus, in older patients with knee OA, tape should be removed and re-applied less frequently than in younger people.
BRACING
A variety of commercial braces are available for knee OA and these differ in terms of price, construction and design. The most simple of designs is a single-piece sleeve made of neoprene and there is evidence to show that this can reduce pain.29–31 An ‘unloader knee brace’ can be used in the setting of unicompartmental OA (Fig. 2). It is a semi-rigid brace, often custom-made, from molded plastic and foam with metal side struts. The design of the brace aims to change the way the force is distributed at the knee by forcing load away from the painful side and biomechanical studies support this load-reducing effect.32,33 Several clinical trials on these braces suggest symptomatic benefits for patients with unicompartmental OA,30,34,35 but the effect may depend upon patient and brace characteristics. Braces were shown to be less effective on obese patients36 and custom-made braces were found to be superior to ‘off the shelf’ designs.37 One of the major barriers limiting the benefits of a brace for knee OA is likely to be adherence. Two studies showed that 42–50% of patients had ceased use of the brace after 6 months.38,39 Factors such as bulkiness, style, ease of application, fit and comfort, are all possible reasons for underlying poor adherence. Given that there is limited research about the effectiveness of knee braces in OA, a brace should not be given as a stand-alone treatment and the decision to provide one should be based on the individual patient response.

INSOLES AND SHOES
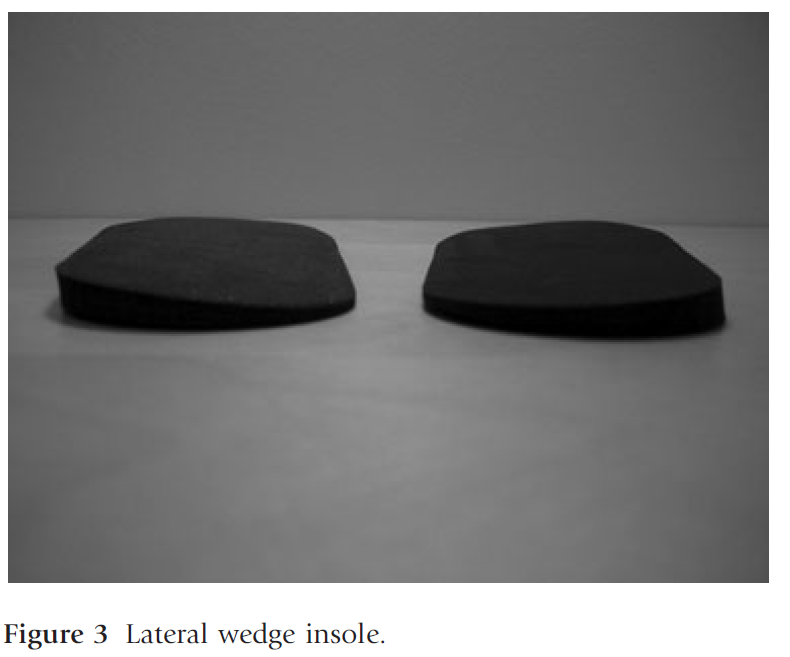
Insoles and footwear offer great potential as simple, inexpensive treatment strategies for knee OA. Lateral wedge insoles have been advocated for medial compartment OA and medial wedge insoles for lateral compartment disease. Given the prevalence of medial compartment OA40 most of the research has been conducted into lateral wedge insoles (Fig. 3). Biomechanical studies show that lateral wedges reduce the adduction moment during walking by 4–12% compared with barefoot or shoes alone in medial knee OA.41–47 This in turn results in a reduction in medial compartment load.48 Research suggests that wedgedesign features such as length and inclination angle may mediate biomechanical effects with full-length insoles42 and a 50–100 tilt41,45 providing the most benefit. Despite evidence for the biomechanical effects of lateral wedges, their use to reduce symptoms of knee OA, including pain, stiffness and function, has not been confirmed in randomized controlled trials. 49–51 It may be that certain subgroups are more likely to respond than others with benefits more likely in those with less severe disease,47 with increased lower lean mass53 and who are younger53 and less
obese.49 Variations in daily usage of wedged insoles may also influence clinical outcome with a nonrandomized trial finding greatest clinical benefits from 5 to 10 h of daily use.54 Footwear has an effect on knee load with recent research suggesting that individual shoe characteristics have an impact.55–58 It appears that flexible footwear56 and shoes with heel height less than 38 mm57 minimize
knee load, whereas stable, more supportive shoes increase knee load.58 There is current interest in designing a shoe to reduce knee load and there are reports of a ‘mobility’ shoe,59 a lateral-wedged sole shoe,60 and a shoe with a variable-stiffness sole.60,61 WhilE there are early results showing that a modified shoe may be of some benefit in reducing symptoms in medial compartment OA,59 no modified shoes specifically for knee OA are commercially available at present.
MANUAL THERAPY
Manual therapy includes many techniques of which the most common is joint mobilization and manipulation. Mobilisation is a manual technique using repetitive passive movement of low velocity and varying amplitudes applied at different points through a range, while manipulation is defined as forceful smallamplitude, high-velocity movements of a joint often applied at the end of the range.62 Manual therapy is commonly used in clinical practice for OA with surveys revealing that 96% of Irish physical therapists63 and 64% of UK therapists64 include it in their management of patients with hip and knee OA, respectively. Despite its common usage, there is little research on the effects of manual therapy for the treatment of knee OA and few studies have evaluated it in isolation from other interventions, such as exercise. The efficiency of manual therapy and exercise in relieving pain and reducing physical disability in knee arthritis was demonstrated in a randomised controlled trial.65 The effect size reported was comparable to that seen following total knee joint arthroplasty. Two studies examining the effect of manual therapy on pain in knee OA demonstrated a hypoalgesia effect supporting a potential pain-relieving benefit of manual therapy.66,67
SUMMARY
There is evidence to indicate that physiotherapy interventions can reduce knee pain and improve function in those with knee OA. Physiotherapy treatments aim to dissipate knee joint load, alter lower limb alignment, improve range of motion and restore normal neuromuscular function. Patients’ responses vary and further research is required to determine which subgroups are most likely to respond to which treatments.No single physiotherapy intervention has shown to provide superior results over the other and it is likely that a combination of treatments is most effective. There is some evidence that physiotherapy in combination with other management strategies, such as weight loss68 and attention to psychological factors69 may provide more significant outcomes than any one of these in isolation. An individual approach to patient management is needed to determine which treatments are most appropriate for each patient.
REFERENCES
1 Conaghan PG, Dickson J, Grant RL (2008) Care and management of osteoarthritis in adults: summary of NICE guidance. BMJ 336, 502–3.
2 Zhang W, Nuki G, Moskowitz RW, et al. (2010) OARSI recommendations for the management of hip and knee osteoarthritis Part III: changes in evidence following systematic cumulative update of research published through January 2009. Osteoarthritis Cartilage 18, 476–99.
3 Brosseau L, Wells G, Tugwell P, et al. (2005) Panel Ottawa: Ottawa panel evidence-based clinical practice guidelines for therapeutic exercises and manual therapy in the management of osteoarthritis. Phys Ther 85, 907– 71.
4 Jordan K, Arden N, Doeherty M, et al. (2003) EULAR recommendations 2003: an evidence based approach to the management of knee osteoarthritis: report of the task force of the standing Committee for International Studies including Therapeutic Trials (ESCISIT). Ann Rheum Dis 62, 1145–55.
5 American Academy of Orthopaedic Surgeons. Clinical guideline on osteoarthritis of the knee 2008 (http://aaos. org/research/guidelines/guide.asp).
6 Altman R, Hochberg M, Moskowitz R, Schnitzer T, et al. (2000) American College of Rheumatology: recommendations for the medical management of osteoarthritis of the hip and knee. 2000 update. Arthritis Rheum 43, 1905–15.
7 Fransen M, McConnell S (2008) Exercise for osteoarthritis of the knee. Cochrane Database Syst Rev (4), Art. No.: CD004376. DOI: 10.1002/14651858.CD004376.pub2. 8 Bartels E, Lund H, Hagen K, Dagfinrud H, Christensen R, Danneskiold-Samsøe B (2007) Aquatic exercise for the treatment of knee and hip osteoarthritis. Cochrane Database Syst Rev (4), Art. No.: CD005523. DOI: 10.1002/ 14651858.CD005523.pub2.
9 Hall KD, Hayes KW, Falconer J (1993) Differential strength decline in patients with osteoarthritis of the knee: revision of a hypothesis. Arthritis Care Res 6, 89–96.
10 Hassan BS, Mockett S, Doherty M (2001) Static postural sway, proprioception, and maximal voluntary quadriceps contraction in patients with knee osteoarthritis and normal control subjects. Ann Rheum Dis 60, 612–8.





