 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Tesla
Tesla Nikola
Nikola Kayser
Kayser Fusion
FusionPHYSIOTHERAPY IN THE INTENSIVE CARE UNIT
- Type: Free
Physiotherapy is reported to be an integral part of patient management in the intensive careunit (ICU) of hospitals in industrialised countries. There is substantial literature whichsupports the role of respiratory management and rehabilitation of critically ill patients,although there is a paucity of randomised controlled trials in this area and trials examiningpatient outcomes. The aims of this review are to present the current evidence for the role ofphysiotherapists in the adult ICU. The efficacy of ‘chest physiotherapy’ on short-term patientphysiological outcomes has been studied extensively and there is moderate-to-strong evidencein support of its role. The safety of physiotherapy treatment in ICU has also recently beenestablished. In addition, there is growing evidence for the role of exercise rehabilitationbeginning in ICU and extending to beyond ICU discharge. Urgent research is required byphysiotherapists to establish the effectiveness of such treatments.
Keywords:Chest physiotherapy, exercise, intensive care, non-invasive ventilation, rehabilitation
Intensive care is a dynamic environment where phys-iotherapists are vital members of the multidiscipli-nary team providing a spectrum of care from acuterespiratory to rehabilitation.The education and training of physiotherapists andtheir role in relation to other health professionalssuch as nurses and respiratory therapists variesgreatly. This withstanding, physiotherapy is reportedto be an integral part of patient management in theintensive care unit (ICU) of hospitals in industrialisedcountries.1The aims of this review are to present thecurrent evidence for the role of physiotherapists in theadult ICU in relation to respiratory managementincluding non-invasive ventilation (NIV), exercise,and short and longer term rehabilitation of patients.Literature searches were performed using the data-bases MEDLINE and CINAHL (cumulated index tonursing and allied health literature) with appropriatesubject headings including intensive care, rehabilita-tion, physiotherapy, physical therapy, critical care,critical illness, chest physiotherapy, manual hyperin-flation and exercise; searches were limited to English language. The reference lists of extracted articles werealso reviewed.Several surveys report on specific physiotherapypractice in the ICU;2–4generally, these are limited torespiratory management. However, the assessmentand management of neurological and musculoskeletalcomplications form an important part of the physio-therapist’s role.1,5It is this individualised, multisystempatient assessment and treatment that defines the roleof physiotherapists compared with respiratory thera-pists and nurses. Physiotherapists may be involvedwith specific patient positioning, suction, mobilisa-tion, exercise, passive movements, manual airwayclearance techniques, manual (MH) and ventilatorhyperinflation (VH), NIV and weaning.1,6–8The coun-try of origin of published research reflects differencesin types of healthcare professionals employed in theICU, with research from the US predominatelyreporting respiratory therapist roles. In the UK, partsof Europe and Canada, South Africa, and Australia,the role of physiotherapists encompasses respiratoryas well as neurological and musculoskeletal patient management.1,8Factors influencing physiotherapyrepresentation in the ICU also include the size of theunit, levels of expertise and staffing, and educationalprofile of physiotherapists.8,9Additionally, the percep-tions of physiotherapy and referral attitudes of inten-sivists may also impact upon their role.7Rationaleand evidence for the role of physiotherapy in refer-ence to the techniques listed above follows withreview under specific subheadings.
CARDIORESPIRATORY MANAGEMENT
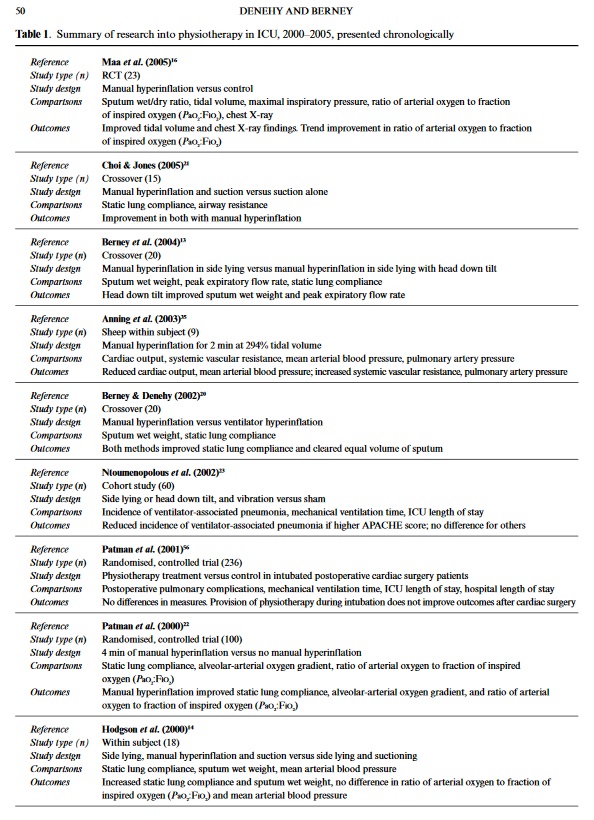
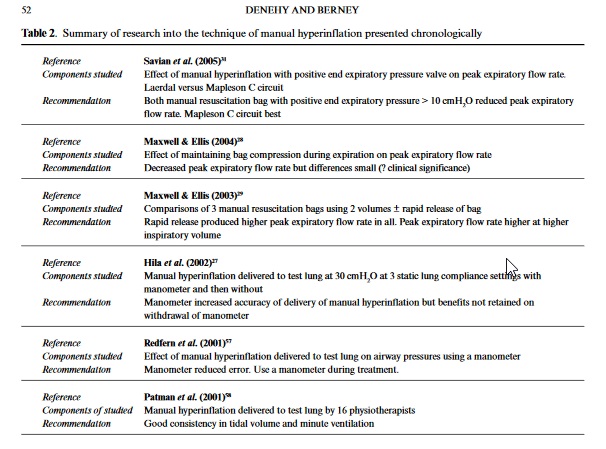
The goals of respiratory physiotherapy managementare to promote secretion clearance, optimise oxygena-tion, improve lung volume and prevent respiratorycomplications in both the intubated and sponta-neously breathing ICU patient.10The rationale fortreatment of intubated patients is based upon theeffects of positive pressure ventilation on respiratoryand cardiovascular systems and the impaired func-tion of the mucociliary escalator.11The resultant dis-turbance of normal secretion clearance potentiallyleads to sputum retention with a subsequent increasein airways’ resistance and work of breathing. Thesepatients are at particular risk as the incidence of ven-tilator-associated pneumonia increases substantiallyfollowing 24 h of mechanical ventilation.12The efficacy of ‘chest physiotherapy’, defined vari-ously as combinations of positioning, MH, VH, andpercussion and vibrations, on short-term patientphysiological outcomes has been studied exten-sively.13–17Table 1 summarises this research for studiesperformed in the last 5 years. There is moderate-to-strong evidence (NHMRC level II and III)18to sug-gest that physiotherapy treatment is effective in:recruiting alveoli;16,19improving secretion clear-ance;13,14compliance;13,14,20airway resistance;21gasexchange;22and reducing the incidence of ventilator-acquired pneumonia.23The technique which has beenincluded in the majority of this research is manualhyperinflation. The most significant finding in rela-tion to ‘chest physiotherapy’ treatment in the ICU isthat it has been found to be safe, with adverse physio-logical changes (APCs) reported in only 29 of 12,800physiotherapy treatments from five Australian ter-tiary hospitals (0.22%).24Several studies have examined the effects of MH onsecretion removal, oxygenation and static pulmonarycompliance. The results have been difficult to inter-pret and compare due to variations in definition ofMH, different circuits that have been used, and incon-sistency in therapists’ technique and treatmentdosage.5,25,26In the last 5 years, several authors have contributed to defining further the technique of MHas used by physiotherapists and added considerableknowledge to the body of literature in this area.13,27–31Summaries and recommendations from their findingsare given in Table 2. For an evaluation of researchprior to 2000, readers are referred to an extensivereview of MH published in 1999.5Beyond this, the use of VH has been compared withMH, and effects on static lung compliance and wetweight of sputum produced have been found to be simi-lar. The use of VH allows the operator to control airwaypressure limits, monitor delivered volumes, and main-tain positive expiratory pressure. This research offerssupport to the use of VH as an alternative to MH, anddescribes the technique of VH.20There is consensus inthe critical care literature supporting the protectiveproperties of positive end expiratory pressure (PEEP) inpreventing ventilator-induced lung injury;32as VH canbe performed without disconnection from PEEP, phys-iotherapists must now consider the potential risks asso-ciated with delivering large tidal volume breaths using amanual resuscitation bag, when potentially the samebenefits can be achieved by using the ventilator.Ntoumenopolous and colleagues23compared phys-iotherapy treatment versus a sham treatment in 60intubated and ventilated critically ill patients. Physio-therapy treatment comprised chest wall vibrationsand specific positioning (no MH). The authors foundthat the incidence of nosocomial pneumonia was 31%less in the group who received physiotherapy,although no difference in time on mechanical ventila-tion or time in the ICU was found. This is the firststudy to compare outcomes for patients of receivingphysiotherapy treatment in the ICU.23This research follows on from previous work by thesame author examining the effect of physiotherapytreatment on nosocomial pneumonia in 46 patients,which found that the more severely ill patients(APACHE 2 score > 15), and those ventilated longerthan 7 days, showed a trend toward benefiting fromphysiotherapy; however, the relatively small samplesize limited the generalisability of this work.17Evidence relating to the cardiovascular and meta-bolic effects of physiotherapy treatment in the ICU isconflicting. Berney and Denehy33found that chestphysiotherapy including ventilator hyperinflation inside-lying did not significantly increase VO2in 20intubated adult ICU patients. This result was not con-sistent with previous similar work;34however, theeffects of physiotherapy treatment on VO2had notpreviously been isolated from those of positioning thepatient and airway suctioning. Providing effectivephysiotherapy management without additional stresson the cardiorespiratory and metabolic systems isvital in critically ill patients.
In several studies performed examining ‘chest phys-iotherapy’ in patient populations, no adverse cardio-vascular consequences have been encountered:13,14,16,33measures of heart rate (HR), cardiac output (CO) andmean arterial blood pressure (MAP) were recordedduring and after physiotherapy including MH inthese studies. Conversely, others have recordedchanges in HR, MAP and pulmonary vascular resis-tance in patients following coronary artery surgery,22and in an animal model.35Comprehensive reviews ofhaemodynamic responses to some aspects of physio-therapy in the ICU are available.36Based upon thefindings outlined above, care must to taken to moni-tor the patient at all times and to treat only if the sta-bility of the cardiovascular system can be maintained.In a recent audit of APC during 12,800 physiotherapytreatments, changes to blood pressure (BP) in patientson inotropes was the most common finding in thesmall number of treatments where APC occurred.24It is important to note that patient demographics inthe studies discussed above did not include acute respi-ratory distress syndrome (ARDS). Recent evidence toprovide lung protective strategies, including moderate-to-high PEEP and low tidal volumes for patients with ARDS also supports the use of periodic recruitmentmanoeuvres to improve oxygenation and reduce mortal-ity.32However, currently, the efficacy of such strategiesmay be limited to patients with non-pulmonary ARDS.37There is an abundance of evidence to support therole of NIV in the ICU in the management of patientswith acute hypercapnic respiratory failure and acutecardiogenic pulmonary oedema; however, contro-versy exists regarding its role in the management ofhypoxaemic respiratory failure.38Recent research sup-ports the use of NIV in the prevention, rather thanthe treatment, of hypoxaemic respiratory failure,where failure to intubate patients may lead toincreased mortality in the NIV group.39Synthesis offindings from the NIV research to date is confoundedbydiffering treatment regimens and the ability of staffto apply the technique effectively. NIV is an evolvingspecialty in ICU which requires specific training andapplication by professionals skilled in patient man-agement. Although the role of physiotherapists in thedecision-making process and application of NIVvaries world-wide, physiotherapists are ideally suited tothis role through their combined skills in physiology,knowledge of equipment and clinical management.
The use of continuous positive airway pressure(CPAP) in preventing intubation in hypoxaemicpatients following abdominal surgery was comparedwith administration of 50% oxygen in 209 patients:those who received CPAP had a lower intubation andpneumonia incidence and a shorter ICU stay.40Findings from this randomised, controlled trial(RCT) support the work of previous authors55andextends the effectiveness of CPAP in influencingimportant outcomes in hypoxaemic patients follow-ing abdominal surgery.In order to contribute further to this growing area,physiotherapists need to become involved in researchinto the role of NIV (including CPAP) in patientmanagement, and to be strong advocates for theirknowledge and ability in its application. Further-more, physiotherapy undergraduate education shouldinclude the principles of management associated withNIV, which can be built upon at postgraduate level
EXERCISE AND REHABILITATION
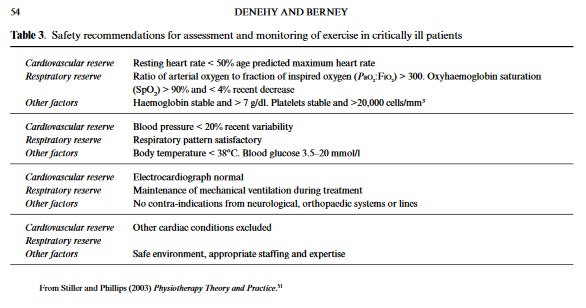
Rehabilitation in the ICU has been defined in a posi-tion paper by The European Respiratory Society as aprocess to achieve optimal daily functioning andhealth-related quality of life of individual patients asmeasured by clinically and/or physiologically relevantoutcome measures.41The methods by which thesebroad aims are achieved vary significantly betweenand even within countries. There is substantial pub-lished literature which supports the role of rehabilita-tion of critically ill patients, although there is apaucity of both randomised controlled trials in thisarea and research examining patient outcomes.25Theprogress of intensive care medicine has dramaticallyimproved survival in critically ill patients;32,42suchimprovement is, however, associated with decondi-tioning, muscle weakness, dyspnoea, depression, anda reduction in quality of life. Ultimately, the goal ofintensive care is quality long-term, rather than short-term survival, but international literature reportspoor quality of life and physical outcomes in ICUsurvivors compared to age-matched controls.43Changes in patient conditions result from pro-longed periods of inactivity, catabolism and drugadministration (e.g. sedative and neuromuscularblocking agents, corticosteroids); these factors con-tribute to weakness that can last for months followingICU discharge.44Severe and prolonged weakness(critical illness neuromyopathy) is present in up to25% of patients mechanically ventilated for greaterthan 7 days.45Critical illness neuromuscular abnor-mality (CINMA) is also an independent predictor of prolonged weaning from mechanical ventilation.46Among treatment strategies including intravenousimmunotherapy, normalising blood glucose and min-imising exposure to drug therapy, physiotherapy hasbeen advocated.45Exercise in the ICU aims tomobilise patients early and facilitate weaning,47opti-mise oxygenation,48and improve function by increas-ing strength and endurance.49The role ofphysiotherapists in the application of exercise varieswidely in response to scant evidence. Primarily, noreliable and valid exercise outcome measure has beendeveloped to aid exercise prescription and measurepatient outcomes, making research in the area diffi-cult. As a result, there are currently no guidelines forrehabilitation of ventilated patients and few trialsinvestigating effectiveness. Jones and colleagues44studied 69 ICU patients at discharge provided with a6-week self-help rehabilitation manual (including aself-directed exercise programme) compared to con-trols (n= 57), and found that scores on the SF-36weresignificantly better for the intervention groupthan controls. There is an urgent need for research byphysiotherapists into the long-term benefits in theterms of physical function and quality of life out-comes of ICU survivors using specifically designedexercise programmes in ICU survivors. Despite thepaucity of evidence, the general consensus is thatrehabilitation should commence as soon as possibleduring ICU admission.For ventilated patients in the ICU, the efficacy anduse of physiotherapy interventions to improve decon-ditioning and weakness is variable. There is limitedevidence that passive stretching is effective in main-taining muscle length or joint range of motion, mostworkhaving been performed using animal models.Furthermore, there are no data reporting the effec-tiveness of splinting to achieve the same aims of treat-ment. Despite this, there is anecdotal evidence thatphysiotherapists still use these techniques: furtherresearch is, therefore, required. The use of the tilttable in long-stay and neurological patients has beenreported by 67% of Australian ICU physiotherapistssurveyed;50the aim of using a tilt table in rehabilita-tion is to re-introduce patients to the vertical position,especially following prolonged immobility. In the sur-vey by Chang and colleagues,5061% of physiothera-pist respondents used tilting less than once per monthor once a year. Reasons given for this were that othertechniques were used in preference (46% of respon-dents), or that it was not clinically indicated (32% ofrespondents). Physiotherapists in high-level ICUs(level 3) used tilting more than in other units, reflect-ing the longer term patient demographics. Theseresults highlight the lack of sound evidence for tiltingcurrently available, and the preference for use of early mobilisation such as assisted standing or marching onthe spot exercise.Mobilisation can refer to many different activities,the exact definition of which are difficult to find.Commonly, there is a hierarchy in accepted mobilisa-tion exercises in the ICU51and this may include bedexercises, sitting over the edge of the bed, standing,transferring, and walking on the spot.52These exer-cise strategies reflect specificity of training for futurefunctional tasks. Mobilising critically ill patientsrequires an initial comprehensive assessment of thepatient’s cardiorespiratory status. Until recently, therehave been no published guidelines for patient safetyand readiness for mobility. Stiller and Phillips51rec-ommend cardiovascular and respiratory parametersto be assessed prior to mobilisation (Table 3) in con-junction with a full patient assessment and use of clin-ical reasoning. The authors subsequently used theseguidelines to study the effects of mobilisation onphysiological parameters in 31 ICU patients andfound that significant increases in HR and BPoccurred during exercise while non-significant reduc-tions in oxyhaemoglobin saturations were recorded.The authors concluded that, using the guidelines pre-viously developed, they were able to institute mobili-sation safely and effectively in the population ofpatients studied. Monitoring during and after exer-cise is vital and recommendations are to observepatient appearance, excessive changes in HR, BPSpO2, ECG arrhythmias, and patient appearance.51Active exercise (including muscle training) has beenshown to improve 6-min walking distance signifi-cantly more than standard care in 80 patients withchronic obstructive pulmonary disease and acute respiratory failure.53The work of Nava53supports theprescription of specific exercises such as bilateral armelevation, hip/knee flexion, and knee extension exer-cises, in addition to functional activities such as sit-to-stand, and walking on the spot, for intubatedcritically ill patients.Whilst the need for exercise rehabilitation in ICUhas been recognised,47there is no clinical research thatidentifies the most effective mode, intensity or fre-quency of exercise prescription. As a result, exercise isapplied by physiotherapists in the ICU using physio-logical principles, underpinned by clinical trainingand a comprehensive understanding of pathophysiol-ogy.Physiotherapists are well placed to provide exer-cise but, again, there is an urgent need for researchinto exercise outcome measurement and the value ofspecific exercise regimens, particularly in intubatedand ventilated patients. In the acutely ill patient, forexample, the value of upper and lower limb strength-ening exercise should be measured together withpatient oxygen demands during and after exercise.
CONCLUSIONS AND RECOMMENDATIONS
Rationalisation of the limited government resourcesto critical care has demanded that physiotherapistsprovide evidence for their continued role in patientmanagement.54Physiotherapy in the ICU needs todemonstrate cost-effective returns. In reviewing theliterature, a lack of randomised clinical trials is evi-dent. Previously, physiotherapists have concentratedon examining the effects of their treatment interven-tions on short-term physiological outcomes: authors attempting to determine the effects of treatment onlonger term outcomes have been limited by smallpatient numbers. The benefits of physiotherapy treat-ment may be better evaluated as a part of a packageof care that includes mobilisation, positioning, andvariable nurse-to-patient ratios. It is plausible thatphysiotherapy treatment as a part of a multidiscipli-nary approach to care is integral in promoting lungrecruitment, reducing the incidence of ventilator-acquired pneumonia, facilitating weaning, and pro-moting safe discharge from the ICU.Obtaining evidence and implementing practiceremain a major barrier for physiotherapists who workin the ICU. Ntoumenopoulos and colleagues23haveprovided sound evidence for the role of physiotherapyin reducing the incidence of nosocomial pneumoniain 60 ICU patients: this research was published in ajournal with a high impact factor. It would be inter-esting to know whether the results have influencedintensivist physiotherapy referral attitudes. Certainly,physiotherapy referral in the unit where this researchwas undertaken has not changed (personal communi-cation) highlighting that implementing change ofpractice based on evidence can be difficult. Given thatnearly 60% of ICU directors from five different coun-tries felt that certain aspects of physiotherapy work(predominately airway clearance) could be covered bynursing staff, it is imperative that physiotherapistspromote their broader clinical role.7Research measuring outcomes will become moreavailable as physiotherapy students embrace a grow-ing research culture in university physiotherapyschools and clinical training facilities,54and morephysiotherapists undertake postgraduate degrees incardiorespiratory specialty areas. Research shouldfocus on the broad aspects of physiotherapy servicedelivery in the ICU as a part of a multidisciplinaryteam using outcomes such as time on mechanical ven-tilation, time in ICU, re-admission to ICU, and dis-charge destination, together with quality of life andmeasures of physical function. Multicentre researchin the form of a randomised controlled trial evaluat-ing the effectiveness of ‘chest physiotherapy’ would beideal, but extremely costly and virtually impossible toimplement due to differences in both medical andphysiotherapy clinical practices and disparity in rolesand autonomy of therapists within ICU environ-ments. In addition, the numbers of patients requiredto find a statistical difference in such a study mean itmost likely will never be performed. Physiotherapymembership of, or recognition by, local critical caresocieties would enhance support and infrastructure toundertake research and help to facilitate changes tophysiotherapy practice in critical care, based upon thebest available evidence.





