 Tecar
Tecar Shock Wave
Shock Wave Plasma
Plasma Laser
Laser Tesla
Tesla Nikola
Nikola Kayser
Kayser Fusion
FusionAn Overview of Shock Wave Therapy in Musculoskeletal Disorders
- Type: Free
shock waves are high-energy acoustic waves generated under water with high voltage explosion and vaporization. Shock wave in urology (lithotripsy) is primarily used to disintegrate urolithiasis, whereas shock wave in orthopedics (orthotripsy) is not used to disintegrate tissues, rather to induce neovascularization, improve blood supply and tissue regeneration. The application of shock wave therapy in certain musculoskeletal disorders has been around for approximately 15 years, and the success rate in non-union of long bone fracture, calcifying tendonitis of the shoulder, lateral epicondylitis of the elbow and proximal plantar fasciitis ranged from 65% to 91%. The complications are low and negligible. Recently, shock wave therapy was extended to treat other conditions including avascular necrosis of femoral head, patellar tendonitis (jumper's knee), osteochondritis dessicans and non-calcifying tendonitis of the shoulder. Shock wave therapy is a novel therapeutic modality without the need of surgery and surgical risks as well as surgical pain. It is convenient and cost-effective. The exact mechanism of shock wave therapy remains unknown. Based on the results of animal studies in our laboratory, it appears that the mechanism of shock waves first stimulates the early expression of angiogenesis-related growth factors including eNOS (endothelial nitric oxide synthase), VEGF (vessel endothelial growth factor) and PCNA (proliferating cell nuclear antigen), then induces the ingrowth of neovascularization that improves blood supply and increases cell proliferation and eventual tissue regeneration to repair tendon or bone tissues. The rise of angiogenic markers occurred in as early as one week and only lasted for approximately 8 weeks, whereas the neovascularization was first noted in 4 weeks and persisted for 12 weeks or longer along with cell proliferation. These findings support the clinical observation that the effect of shock wave therapy appears to be dose-dependent and symptom improvement with time. Additional information including the cellular and molecular changes after shock wave therapy are needed for further clarification on the mechanism of shock wave therapy in musculoskeletal system.
Key words: shock wave therapy, musculoskeletal system, mechanism
Historic background
During World War II, engineers from Dornier factory (Germany) had observed the patterns of injuries in tank crews when the turrets were struck by shell, and pitting of metal surfaces was observed associated with supersonic flight. The influence of shock wave on human tissue was first documented when the lung tissue of castaways was disrupted because of the explosion of water bombs even though no external symptoms of violence existed. The wife of one engineer suggested the possible application of this knowledge to fragmentation of kidney stones and this idea had led to the development of lithotripsy in mid 1970 in Munich, Germany. The interaction between shock waves and biologic tissues in animals were investigated in Germany between 1968 and 1971. In 1974, a research grant "Application of Extracorporeal Shock Wave Lithotripsy" was approved. The first patient with kidney stone was treated with shock wave in Munich, Germany (Dornier lithotriptor HM1) in 1980. In 1983, the first commercial lithotriptor (HM3, Dornier) was installed in Stuttgart, Germany. The first case of gallstone treated with ESWL was performed in Munich, Germany in 1985. Twenty some years later, lithotripsy has become the gold standard for the initial treatment of urolithiasis. In musculoskeletal system, the application of shock waves to the loosening of cement in the revision of total hip was thought to be feasible at that time. Karpman RR et al(3) performed a study in canine femoral model, and demonstrated microfractures within the bone cement and a definite disturbance of the bone/cement interface when the specimens were examined with scanning electron microscopy and reflected light microscopy. Using the same principles, other authors reported the potential use of shock wave for bone cement removal. In mid 1980, incidental observations during animal studies found an osteoblastic response pattern that generated an interest in the potential application of extracorporeal shock wave therapy to numerous orthopedic disorders.In the past 10 to 15 years, shock wave therapy had shown effects in the treatment of certain orthopedic disorders including nonunion of long bone fractures, calcific tendinitis of the shoulder, lateral epicondylitis of the elbow and proximal plantar fasciitis. More recently, several studies had extended shock wave therapy to patellar tendinits (jumper's knee), osteochondritis dessicans and avascular necrosis of the femoral head and had shown satisfactory results. The use of extracorporeal shock wave therapy has gained significant acceptance in Europe, especially Germany, Austria, Italy and in Taiwan, and has led to the change of European Society for Musculoskeletal Shockwave Therapy to International Society for Musculoskeletal Shockwave Therapy (ISMST) in 2000. In USA, FDA (Food and Drug Administration) approved in Oct 2000 on specific shock wave device (OssaTron, High Medical Technology, Lengwil, Switzerland) for the indication of proximal plantar fasciitis, with many other clinical trials under study including lateral epicondylitis of the elbow, calcific tendinitis of the shoulder, non-union of fracture. Based on our extensive clinical results in the past 3 to 4 years, and the innovative findings on the mechanism of shock wave therapy, the Department of Health of Taiwan Government had approved the OssaTron shock wave therapy for patients with proximal plantar fasciitis in May 2001, with conditional approval on several other orthopedic conditions including tendinitis of the shoulder, lateral epicondylitis of the elbow and non-union of long bone fractures. In the past, the Annual Congress of The International Society of Musculoskeletal Shockwave Therapy (ISMST) was traditionally held in European countries and cities including Izmir, Turkey in 1998, London, England in 1999, Naples, Italy in 2000, Munich, Germany in 2001, Winterhur, Switzerland in 2002. The first ISMST Congress outside the Europe was held in Orlando, Florida, USA in February 2003. During the general meeting of the association members from 34 countries, I was elected as the new president of the association. The Managing Board of ISMST has decided to hold the 7th Annual Congress of ISMST meeting in Kaohsiung, Taiwan in April 2004.
Principle of shock wave therapy
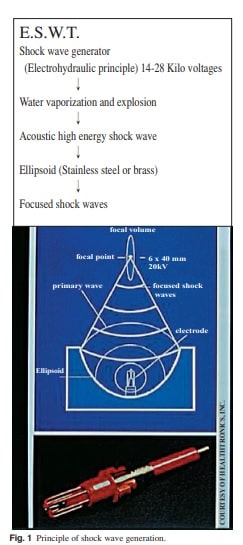
Shock waves are generated by an underwater high-voltage condenser spark discharge and then focused at the diseased area, using an elliptical
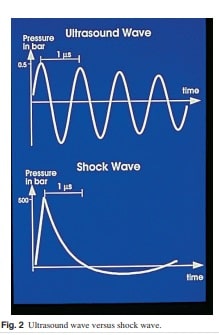
reflector (Fig. 1).(7,29,30) Shock waves are high amplitude sound waves from a transient pressure disturbance that propagate in three-dimension space with a sudden rise from ambient pressure to its maximum pressure at the wave front. A shock wave is a sonic pulse that has certain physical characteristics. There is an initial rise of a high peak pressure, sometimes more than 100 MPa (500 bar) within less than 10 ns
(nanoseconds), followed with a low tensile amplitude (up to 10 MPa), a short life cycle of approximately 10 µs and a broad frequency spectrum in the range of 16 to 20 MHz. There are two basic effects of shock waves: the primary effect is direct generation of mechanical forces that result in the maximally beneficial pulse energy concentrated at the point.
where treatment is to be provided; and the secondary effect is the indirect mechanical forces by cavitation which may cause negative effect or damage to the tissues. Shock wave differs from ultrasound wave that is typically biphasic and has a peak pressure of 0.5 bar (Fig 2). In essence, the peak pressure of shock wave is approximately 1000 times that of ultrasound wave. Shock waves change their physical properties through attenuation and steepening when traveling
through a medium and through reflection and refraction at the boundaries when subsequently moving into another medium. At the boundary layer between two media one part of an approaching shock wave will be reflected and the other part will be transmitted. Losses through attenuation in water are approximately 1000 times lower than an air. Shock waves are generated within water and subsequently transferred to the human body by means of a contact medium. These ensure small losses attribut
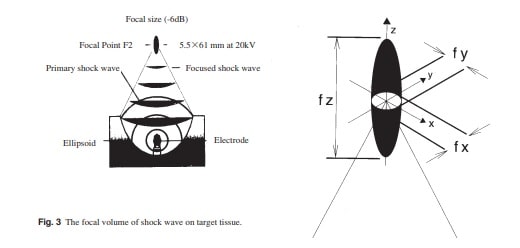
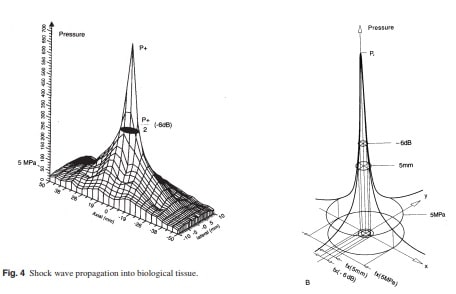
able to attenuation and reflection by any boundary area, and the energy of shock wave will be concentrated in the treatment focus. It is along the boundaries between different media such as muscle and bone or lung tissue that the sound field experiences the biggest changes and emits the highest energy, and where the most biologic effects are expected. The focal volume of shock wave on target tissue is shown in Fig. 3. Shock wave pressure (in MegaPascals) measures the tensile force with fiberoptic hydrophone. Energy flux density describes the maximum amount of acoustic energy that is transmitted through an area of 1 mm2 per pulse. The energy describes the total acoustical energy per released shock wave. Therefore, the total energy is the accumulated energy flux density as they integrated over the entire region. In addition to the primary focal point, a second focal point (6dB) is defined the volume area of tissue within which the pressure is at least 1/2 its peak pressure. Shock wave propagation into biological tissue is shown in Fig. 4.
Methods of shock wave generation
There are three main techniques through which shock waves are generated. These are the electrohydraulic, electromagnetic, and piezoelectric principles, each of which represents a different technique of generating the shock wave. All involve the conversion of electrical energy to mechanical energy. Shock wave generation through the electrohydraulic principle represents the first generation of orthopedic shock wave machine. It is characterized by large axial diameters of the focal volume and high total energy within that volume. Shock wave generation through the electromagnetic technique involves the electric current passing through a coil to produce a strong magnetic field. A lens is used to
focus the wave, with the focal therapeutic point being defined by the length of the lens. The amplitude of the focused waves increases by non-linearity when the acoustic wave propagates toward the focal point.(1,30) Shock wave of piezoelectric technique involves a large number (usually > 1000) of piezocrystals mounted in a sphere and receives a rapid electrical discharge that induces a pressure pulse in the surrounding water steepening to a shock wave. The arrangements of the crystals cause selffocusing of the wave toward the center (target), and lead to an extremely precise focusing and high-energy within a defined focal volume.(1) When comparing different shock wave devices, the important parameters include pressure distribution, energy density and the total energy at the second focal point in addition to the principle of shock wave generation of each device.
The processes that shock waves induced in biologic tissue are not fully understood, especially as they relate to the induction of bone healing. The most important physical parameters of shock wave therapy for the treatment of orthopedic disorders include the pressure distribution, energy density and the total acoustic energy.(1,30,33) In contrast to lithotripsy in which shock waves disintegrate renal stones, shock waves are not being used to disintegrate tissue, but rather to microscopically cause interstitial and extracellular responses.(1,30) Currently, the therapeutic mechanism of shock wave therapy in musculoskeletal problems and the specific biologic effects on the various tissues (bone, cartilage, tendon and ligament) are not fully understood. The effects from direct
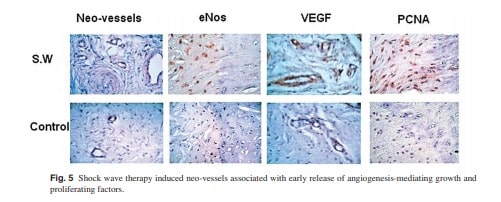
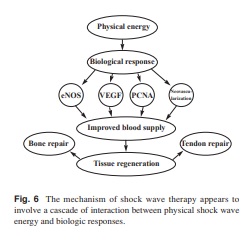
forces and cavitation from indirect forces cause trabecular microfractures or interstitial gaps and hematoma formation, as well as focal cell death, which then stimulate new bone or tissue formation.(1,30,34-38) When shock waves hit the cortical bone, 65% are transmitted and 35% reflected. The maximum stimulation of osteogenesis occurs at the interface of cortical and cancellous bones, while the tensile waves cause cavitation and osteocyte death, followed by osteoblast migration and new bone formation. The exact mechanism of shock wave therapy remains unknown. Some authors hypothetically described that shock waves cause microfracture or micro-trauma and hematoma formation that eventually lead to osteoblastic activities, increased callus formation and bone healing.(1,7,8,30,35,36) Others postulated that shock wave therapy relieves pain due to insertional tendinopathy by provoking painful level of hyper-stimulation analgesia. Recently, the results of our animal experiments demonstrated that shock wave therapy induces neovascularization at the tendon-bone junction associated with the early release of angiogenesis-mediating growth and proliferating factors including eNOS (endothelial nitric oxide synthase), VEGF (vessel endothelial growth factor) and PCNA (proliferating cell antinuclear antigen) that lead to improvement of blood supply and tissue regeneration (Fig. 5).(21,47) Therefore, the mechanism of shock wave therapy appears to involve a cascade of interaction between physical shock wave energy and biologic responses as shown in Fig. 6.
Shock wave therapy in orthopedic disorders
In 1986, Haupt reported the first experiment to investigate the influence of shock wave on bone.(9) The first shock wave treatment for non-union of fracture was done in Bochum, Germany in 1988. In the same year, Valchanov and Michalilov described shock wave therapy for non-unions and delayed unions, and reported a success rate of treatment of 85% despite the poor control study. The first report of shock wave therapy on calcific tendonitis of the shoulder was made in 1990, with subsequent reports on lateral epicondylitis and plantar fasciitis. The first orthopedic shock wave machine (OssaTron, HMT AG, Lengwil, Switzerland) was made available in 1993. As of 2002, the ISMST recommended the following indications for shock wave therapy in orthopedic disorders. These included nonunions and delayed unions of long bone fractures, calcific tendonitis of the shoulder, lateral epicondylitis of the elbow and proximal plantar fasciitis. In addition, the effects of shock wave therapy were investigated on several other conditions including avascular necrosis of the femoral head in adults, osteochondritis dessicans of the talus and the knee, patellar tendonitis, Achilles tendonitis, medial epicondylitis of the elbow, trochanteric bursitis and noncalcific tendonitis of the shoulder.
Animal experiments
Shock wave therapy versus bone healing Several studies had investigated the effects of shock wave therapy on fracture healing and its effects on other musculoskeletal tissues including cartilage in animal experiments. Haupt et al(48) in an experimental model in rats, confirmed a positive effect of shock wave treatment on fracture healing. Johannes et al(60) showed the promotion of bony union with shock wave therapy in hypertrophic non-unions in dogs. Wang et al(57) demonstrated that shock wave therapy enhanced callus formation and induced cortical bone formation in acute fractures in dogs at 12 weeks, and the effect of shock wave therapy seemed to be time dependent. Wang FS et al(61)
had successfully created a non-union model in rats, and had shown that shock wave therapy significantly promotes fracture healing than the control.
However, Forriol et al(62) reached an alternative conclusion and thought that shock wave treatment might delay bone healing and did not recommend its use in clinical orthopedics. Therefore, there are conflicting results on the effect of shock wave therapy on bone healing in animal experiments. Most studies showed a positive effect of shock wave therapy on fracture healing,(48,60,61) whereas only one study showed a negative result.(62) The possible reasons for the discrepancy included the different types of animals and the different shock wave energy flux densities used in different studies.
Wang et al had demonstrated that high-energy shock wave therapy produces a significantly higher bone mass including BMD (bone mineral density), callus size, ash and calcium contents, and better bone strength including peak load, peak stress and modulus of elasticity than the control group after fractures of the femurs in rabbits. However, the effects of low-energy shock wave therapy were less prevailing with comparable results as compared with the control. Therefore, the effect of shock wave therapy on bone mass and bone strength appeared to be dosedependent and progression with time. There are many other studies investigating the effect of shock wave therapy on bone healing in animals. The important findings included superoxide mediates shock wave induction of ERK-dependent osteogenic transcription factor (CBFA-1) and mesenchymal cells differentiation toward osteoprogenitors.(64) Extracorporeal shockwave promotes bone marrow stromal cell growth and differentiation toward osteoprogenitors associated with TGF-β1 and VEGF induction.(47) Physical shock wave mediates membrane hyperpolarization and Ras activation for osteogenesis in human bone marrow stromal cells.(63) Shock wave enhances fracture healing and biomechanical strength associated with increase in TGF-β1 induction.(65) Altered expression of bone morphogenetic protein in shockwave promoted healing of fracture defect.
Shock wave therapy versus insertional tendinopathy at the tendon-bone junction Many studies were devoted to investigate the effect of shock wave therapy on insertional tendinopathies at the tendon-bone junction.(11,20,23,28,31,32,54,66-68) Rompe et al.(54) demonstrated
dose-related effects of shock waves on rabbit tendo Achilles, and suggested that energy flux density of more than 0.28 mJ/mm2 should not be used clinically in the treatment of tendon disorders. In their study, a statistically significant increase of capillary formation was noted with higher energy shock wave (0.60 mJ/mm2 ), which also caused more tissue reaction and potential damage to the tendon tissue. Wang et al(21)
had demonstrated that low energy shock waves enhance neovascularization with formation of new capillary and muscularized vessels at the tendonbone junction of the Achilles tendons in dogs. In a study in rabbit model, Wang et al further demonstrated that shock wave therapy induces a significantly higher number of neo-vessels (neovascularization) including capillary and muscularized vessels than the control without shock wave therapy at the tendonbone junction. In the earlier stage, shock wave therapy releases a higher number of angiogenesis-mediating growth and proliferating indicators including eNOS, VEGF, and PCNA than the control without shock wave therapy. The eNOS and VEGF began to rise in as early as one week and remained high for 8 weeks, then declined in 12 weeks; whereas the increase of PCNA and neo-vessels began in 4 weeks and persisted for 12 weeks and longer. Therefore, the mechanism of shock wave therapy may have involved the early release of agniogenesis-related growth factors, which in turn induce neovascularization and improve blood supply at the tendon-bone junction of the Achilles tendon in rabbits. It is believed that the mechanism of shock wave therapy alleviates pain due to insertional tendinopathy by the induction of neovascularization and improvement of blood supply to the tissue, and initiating repairs of the chronically inflamed tissues by tissue regeneration.
Clinical applications
Non-union and delayed union of long bone fracture Several studies on the effect of shock wave ther-apy for non-union and delayed union of long bone fractures, and reported the success rate ranged from 50% to 90%. Wang et al(19) treated 72 patients with non-unions of long bone fracture with shock wave therapy, and reported a 49% success rate of bony union associated with complete resolution of pain and functional recovery at initial 3-month follow-up of 55 patients; the success rate of bony union was 82.4% at 6-month follow-up of 34 patients; and the success rate of bony union was 88% (22/25) at 9 to 12 month follow-up in 22 patients. Schleberger and Senge(75) showed successful fracture healing in three of four pseudoarthroses treated with 2000 shock waves. Valchanou et al(17) reported bony unions in 70 of 82 patients with delayed or chronic nonunion of fractures at various locations. Rompe et al(73,74) reported a 50% success rate in the treatment of delayed bone union with shock waves in another clinical study, whereas Vogel et al(18) reported a 60.4% union rate in 48 patients with pseudarthroses treated with 3000 shock wave impulses. Schaden et al(16) reported a success of 85% in the treatment of 115 delayed and non-unions.
Proximal plantar fasciitis
Many studies were performed to investigate the effect of shock wave therapy on patients with proximal plantar fasciitis and reported a success rate ranging from 34% to 88%.(10,13,24,28,76,77) Wang et al(24,25) treated 79 patients (85 heels) with plantar fasciitis including 59 women and 20 men with an average age of 47 years (range 15-75) with shock wave therapy with on one-year follow-up. The overall results were 75.3% complaints free, 18.8% significantly better, 5.9% slightly better and none unchanged or worse. The recurrent rate was 5%. It was concluded that shockwave therapy is a safe and effective modality in the treatment of patients with proximal plantar fasciitis. Rompe et al(77) compared the results of 15 patients with painful heels treated with 1000 impulses of shockwaves at 0.06 mJ/mm2 given three times at weekly intervals with the results in an equal number of patients treated with placebo and concluded there was significant alleviation of pain and improvement of function in shockwave treated patients.
Calcifying tendinitis of the shoulder
The success rate of shock wave therapy on patients with calcific tendinitis of the shoulder was reported ranging from 47% to 70%. Wang et al(22,23) compared the results of shock wave therapy on 37 patients (39 shoulders) with calcific tendonitis of the shoulder with a control group of 6 patients (6 shoulders). The overall results of the shock wave group were complaints free in 60.6%, significantly better in 30.3%, slightly better in 3.0% and unchanged in 6.1%. Only two patients (6%) showed recurrent pain of lesser intensity, and none showed worse symptoms. The results of the control group were slightly better in 1 (16.7%) and unchanged in 5 (83.3%). Radiographs showed complete elimination of calcium deposits in 57.6%, partial elimination or fragmentation in 15.1%, and unchanged in 27.3% for the shock wave group. For the control group, the calcium deposit was fragmented in 1 (16.7%) and unchanged in 5 (83.3%). None showed recurrence of calcium deposit two years after shock wave therapy. There was a correlation of functional improvement with the elimination of calcium deposit. Spindler et al(82) reported complete pain relief and full shoulder joint movement in three patients two years after shock wave therapy, and a fragmentation of calcification was achieved after 24 hours. Loew and Jurgowski(78) treated 20 patients with two sessions of 2000 impulses each of shock wave and reported a marked reduction of symptoms with an average of 30% improvement in the Constant score at the 12-week follow-up. Radiographs showed complete elimination of the calcification in seven patients, and partial elimination in five patients. Magnetic resonance imaging did not show any lasting damage to bone or soft tissue. Rompe et al(80,81) reported significant improvement of subjective and objective criteria, in which 72.5% of the patients had no or only occasional discomfort, and only six (15%) of 40 patients treated with 1500 shock waves reported no improvement. Complete or partial disintegration of the calcium deposits was observed in 62.5% of the patients. In another study, Rompe et al(15) demonstrated that shock wave therapy provides equal or better results than surgery in patients with calcifying tendonitis of the shoulder.
Lateral epicondylitis of the elbow
Many studies investigated the effect of shock wave therapy on patients with lateral epicondylitis of the elbow, and reported the success rate ranging from 48% to 73%. Wang et al(86) compared the results of shock wave therapy on 57 patients (58 elbows) with lateral epicondylitis of the elbow with a control group of 6 patients (6 elbows) with a followup of 12 to 26 months. The overall results of the treatment group were complaints free in 27 (61.4)%, significantly better in 13 (29.5)%, slightly better in 3 (6.8%) and unchanged in 1 (2.3%). Recurrent pain of lesser intensity was noted in 3 patients (6.8%). In the control group, however, the results were unchanged in all 6 patients. Rompe et al(84,85) reported good or excellent outcome in 48% and an acceptable results in 42% at the final review in 24 weeks in 50 patients with chronic tennis elbow treated with 3000 impulses of shock wave therapy compared with 6% and 24%, respectively, in patients treated with 30 impulses.
Other New clinical applications
AVNFH (avascular necrosis of the femoral head) in adults There were publications on the effect of shock wave therapy for avascular necrosis of the femoral head in adult. Ludwig et al(25) reported comparable clinical results of shock wave therapy in the treatment of patients with early stages (I to III) of AVNFH(87,88). Complete resolution of the disorder was confirmed with MRI study in selected cases. Our preliminary results of shock wave therapy in 18 patients (22 hips) with early stages of AVNFH showed significant improvement in pain scores and Harris hip scores with 3 to 6 month follow-up. MRI of the hip taken in 6 months after shock wave therapy showed significant reduction of bone marrow edema despite insignificant interval change in the size of the lesion. Longer follow-up is needed to validate the effect of shock wave therapy on patients with early stages of AVNFH.
Osteochondritis dessicans
Several studies reported the high success rate of shock wave therapy in patients with osteochondritis dessicans in the knee and the ankle.(27,55) The effect on osteochondritis dessicans appears to correlate with the age of the patients and the size of the lesion. Additional information with larger number of patient population and longer follow-up are needed to vali date the clinical indication of shock wave therapy on osteochondritis dessicans or osteochondral lesion.
Jumper's knee (Patellar tendonitis)
Recent studies reported favorable results of shock wave therapy in athletes with Jumper's knee (patellar tendonitis)(27,55). This indication is being extended to patients with donor site pain due to patellar tendinitis after harvesting the patellar tendon for ACL reconstruction. The preliminary results of shock wave therapy in 10 athletic patients with the diagnosis of primary jumper's knee and ACL graft related complications showed improvement of pain in 80% of the cases (unpublished). Additional studies with a larger number of patient population and longer follow-up are in progress.
Other conditions
The indications for shock wave therapy in orthopedic disorders continue to expand with time and experience. Few studies reported a positive influence of shock waves on malignant cells, and the potential of gene therapy.(36,89-91) This has opened a door that shock wave therapy may be applied in the treatment of other conditions including tumors. In conclusion, shock wave therapy in orthopedics (Orthotripsy) differs from lithotripsy for urolithiasis. In lithotripsy, shock waves disintegrate renal stones. However, shock waves in orthopedics were not being used to disintegrate tissues, rather promote promoting biological responses including tissue regeneration. Although the exact mechanism of shock wave therapy remains unknown, the results of our animal experiments had shown a cascade of reaction from physical shock wave energy to the biologic responses including the early release of agniogenesis-mediating growth factors within one week, followed by the promotion of neovascularization, improved blood supply and tissue proliferation in 4 weeks, and initiating the repair for chronically inflamed tendons by tissue regeneration. Shock wave therapy in orthopedics is a new therapeutic modality with effectiveness, convenience and safety. The complication rates are low and there is no devicerelated problem. It is has the potential of replacing surgery on certain orthopedic disorders without surgical risks.
reference
An Overview of Shock Wave Therapy in Musculoskeletal Disorders





